→Isoflurane: thanks |
|||
| Line 323: | Line 323: | ||
:::My guess is that the reviewers (whose efforts I sincerely and deeply appreciate) are only looking at their assigned articles. This means that we're likely to have to explain the same issues to each one, individually, at each and every article, instead of having a centralized communication point for them. In the meantime, I suspect that we need to get a few more people to watchlist some or all of the articles. [[User:WhatamIdoing|WhatamIdoing]] ([[User talk:WhatamIdoing|talk]]) 03:09, 10 May 2010 (UTC) |
:::My guess is that the reviewers (whose efforts I sincerely and deeply appreciate) are only looking at their assigned articles. This means that we're likely to have to explain the same issues to each one, individually, at each and every article, instead of having a centralized communication point for them. In the meantime, I suspect that we need to get a few more people to watchlist some or all of the articles. [[User:WhatamIdoing|WhatamIdoing]] ([[User talk:WhatamIdoing|talk]]) 03:09, 10 May 2010 (UTC) |
||
::::Good idea to get more people to watchlist the articles - but seems like a laborious way to check, for the long haul. Regarding transparency of communication, I posted at the project talk page [http://en.wikipedia.org/wiki/Wikipedia_talk:WikiProject_Medicine/Google_Project] asking TimV how he's communicating with the editors. I'm not sure if that's the best way to contact him about it, though.[[User:Postpostmod|Postpostmod]] ([[User talk:Postpostmod|talk]]) 13:00, 10 May 2010 (UTC) |
::::Good idea to get more people to watchlist the articles - but seems like a laborious way to check, for the long haul. Regarding transparency of communication, I posted at the project talk page [http://en.wikipedia.org/wiki/Wikipedia_talk:WikiProject_Medicine/Google_Project] asking TimV how he's communicating with the editors. I'm not sure if that's the best way to contact him about it, though.[[User:Postpostmod|Postpostmod]] ([[User talk:Postpostmod|talk]]) 13:00, 10 May 2010 (UTC) |
||
:::::Hello everyone, I'm one of those editors, but I am contracted for BioscienceWriters.com (BSW) not AJE. I think those are the only two companies involved right now, but don't quote me on that. BSW just started a trial of 20 articles all from the list on the [http://en.wikipedia.org/wiki/Wikipedia_talk:WikiProject_Medicine/Google_Project] page. AJE has been reviewing project articles for longer than we have, but that is all I know about their participation. My understanding is that BSW is doing trials edits for about 20 articles and if our reviews are useful to you, there may be a contract for a larger number of articles in the future. The trial review process should take a couple of weeks. We were directed to spend about 2 hours per article, minimize direct edits unless they are simple (like adding citations or citation needed tags) and focus on these areas in order of priority: |
|||
:::::*the first priority is to point out inaccuracies |
|||
:::::*the second is probably to point out important missing information |
|||
:::::*the third is to focus on more complete citations |
|||
:::::But collaborative organization is as follows: a google representative and a [http://en.wikipedia.org/wiki/Wikipedia_talk:WikiProject_Medicine/Google_Project] representative (TimV) gave us a brief intro via phone conference call, and now all the editors post questions and requests for feedback either to the BSW business manager or directly on the [http://en.wikipedia.org/wiki/Wikipedia_talk:WikiProject_Medicine/Google_Project] talk page. The BSW manager communicates with the Google and Wiki rep and then gives us feedback. So in essence, we are getting feedback both directly from you via the [http://en.wikipedia.org/wiki/Wikipedia_talk:WikiProject_Medicine/Google_Project] talk page and indirectly from TimV and a Google representative. I encourage you to communicate your needs and thoughts on the reviews on the [http://en.wikipedia.org/wiki/Wikipedia_talk:WikiProject_Medicine/Google_Project] talk page and because everyone is reading those. The one discrepancy I've noticed is that talk page participants seem to like more direct edits, while our direction from the project organizers is to minimize those. So I am trying to do a balance between those needs. And yes, Google is footing the cost of the project. Google is also definitely reading that talk page and taking note of your comments there, so make them known! Not sure about this one. Should I cross post this on the project page? [[User:BSW-RMH|BSW-RMH]] ([[User talk:BSW-RMH|talk]]) 15:27, 13 May 2010 (UTC) |
|||
== [[Münchausen by Internet]] == |
== [[Münchausen by Internet]] == |
||
Revision as of 15:27, 13 May 2010
Welcome to the WikiProject Medicine talk page. If you have comments or believe something can be improved, feel free to post. Also feel free to introduce yourself if you plan on becoming an active editor!
We do not provide medical advice; please see a health professional.
- Unsure about something? Make sure to look at our style and source guidelines.
- Please don't shout, remain civil, be respectful to all, and assume good faith.
- Put new text under old text. Click here to start a new topic.
- Please sign and date your posts by typing four tildes (
~~~~). - Threads older than 10 days are automatically archived.
- Please see Wikipedia:WikiProject_Medicine/Newsletter/Mailing_list
| List of archives | |
|---|---|
|
List of causes of... articles
Are lists such as List of causes of diarrhea and List of causes of fever acceptable topics? Tim Vickers (talk) 20:07, 23 February 2010 (UTC)
- They're fundamentally lists of differential diagnoses, and as such, I think they're sourceable (and therefore probably WP:Notable). Whether they're really desirable is a different story.
- Another proposed approach is to add an external link to an outside list, as discussed above. An external link has the advantage of being less work for us, and the disadvantage of not taking readers to the Wikipedia articles about the individual ddxes. WhatamIdoing (talk) 20:26, 23 February 2010 (UTC)
I feel that the lists are desirable, as they are typically fairly comprehensive, provide references, and educate the reader. Immunize (talk) 20:56, 23 February 2010 (UTC)
- I do not think we can do these lists well and therefore they think they should be discourage. Have suggested as WIAD mentioned that we add a link to DiagnosisPro which does an excellent job of differentials and does by the way take suggestion. Than possibly get rid of all these lists. Template_talk:Infobox_symptom#Differential_diagnosis. I recommend that when writing articles about signs and symptoms that rather than writing the differential in list form we provide a brief summary of each condition mentioned such as has been done at limp and testicular pain.Doc James (talk · contribs · email) 20:58, 23 February 2010 (UTC)
Why not use DiagnosisPro as a source, rather then adding an external link and then mass-deleting lists? Immunize (talk) 21:10, 23 February 2010 (UTC)
- Problems with using DP extensively as a source is copyright issues as this would basically be a cut and past. How many of these lists do we have? I am suggested to keep the info in article and expand each to a brief summary of the condition with hopefully comments on the relative prevalence of different condition in the DD.Doc James (talk · contribs · email) 21:15, 23 February 2010 (UTC)
- (ec) I think the problem with these articles is that, from my perspective, they sort of encourage people to use WP for medical advice. If people want to look up diarrhoea, they go to the diarrhoea article, but people with those symptoms who want to look it up could often go to one of these lists to find out what is causing it, and misunderstand something or get worried, partly because it is out of context. IMO, I think these are only desirable if they provide sufficient context and additional information, for example the prevalence of the conditions, rather than just a list, as one would find if it were part of the main article. Jhbuk (talk) 21:11, 23 February 2010 (UTC)
It already states that WP should not be used for medical advice, but if you feel it is still an issue, I would suggest putting a statement on every list of symptom causes explicitly stating that this list should not be used as medical advice. We could even create a template for this purpose. Immunize (talk) 21:20, 23 February 2010 (UTC)
- Wikipedia:No disclaimers in articles: A disclaimer is neither necessary nor appropriate. WhatamIdoing (talk) 22:08, 23 February 2010 (UTC)
- Yes. My point was really more that these types of article specifically are probably more prone to people using them for advice than with most articles, and that they could do more harm than good if we don't put the information in context. Jhbuk (talk) 22:18, 23 February 2010 (UTC)
All lists should be merged with their parent articles. If a cause for diarrhoea is not worth mentioning on diarrhea, it is probably not notable for the list either. JFW | T@lk 22:49, 23 February 2010 (UTC)
- I agree with JFW and that without appropriate context these lists should probably be deleted not cut and pasted and moved over to the main article.Doc James (talk · contribs · email) 23:09, 23 February 2010 (UTC)
I was not aware that disclaimers were not allowed on articles, but does a template really count as a disclaimer if is says sometinhing like "not intended as medical advice"? Immunize (talk) 23:15, 23 February 2010 (UTC)
- Yes that would count as a disclaimer. Doc James (talk · contribs · email) 23:19, 23 February 2010 (UTC)
Also, I feel that if the lists cannot remain in there current form, they should be merged into there parent articles not deleted. For instance, I feel list of causes of fever should be merged into Fever, which has only a short causes section. However I still feel that it would be best for the lists to remain in there current form. Yes, there is a risk that these pages could be taken as advice, but we have an appropriate disclamier that should dissuade this use of the lists here. Immunize (talk) 23:26, 23 February 2010 (UTC)
- I have no concerns about this being health advice. My concern is I do not think large lists of differentials are encyclopedic. There are 744 causes of abdo pain [1] 1089 causes for fever [2]. This IMO is not what we should be doing. Others do it so much better and we should just link to them than do what we are here for WP:ENC. Doc James (talk · contribs · email) 23:33, 23 February 2010 (UTC)
- Completely agree wrt encyclopaedic purpose. It would be encyclopaedic to indicate common causes in the parent articles. Listing all possible causes dilutes the value of the list so it becomes a pointless exercise. Colin°Talk 09:16, 24 February 2010 (UTC)
- I agree completely: much better to add a external link.--Garrondo (talk) 11:05, 24 February 2010 (UTC)
- Completely agree wrt encyclopaedic purpose. It would be encyclopaedic to indicate common causes in the parent articles. Listing all possible causes dilutes the value of the list so it becomes a pointless exercise. Colin°Talk 09:16, 24 February 2010 (UTC)
- I have no concerns about this being health advice. My concern is I do not think large lists of differentials are encyclopedic. There are 744 causes of abdo pain [1] 1089 causes for fever [2]. This IMO is not what we should be doing. Others do it so much better and we should just link to them than do what we are here for WP:ENC. Doc James (talk · contribs · email) 23:33, 23 February 2010 (UTC)
I completely disagree. As WhatamIdoing (talk · contribs) said, these lists are notable, and most of the lists are well sourced (for instance, in my list of causes of fever, each disease listed has a reference that certifies that it can cause fever, so they are well sourced and meet WP:NOTABLE guidelines. Best wishes. Immunize (talk) 14:45, 24 February 2010 (UTC)
- We have no notability guideline for lists; WP:NOTABLE is irrelevant to this discussion. The consensus here is that these lists in their present form (a bare list that mixes the exotic with the commonplace) are pointless. I see from your talk page that you have assumed that since other such lists haven't been deleted that they are therefore useful. Our Deletion policy wouldn't delete such a list but don't confuse that with whether the list has merit. Colin°Talk 21:22, 24 February 2010 (UTC)
- No, I said that the lists are probably WP:Notable; I make no definitive or authoritative statement, because, as Colin indicates, there are no simple rules for determining notability for lists. Even if the subject of the list is accepted, notable subjects are not required to be kept as separate articles.
- Additionally, a laundry list may be less useful for our readers than an explanation. Take fever as an example: nearly all fevers are caused by infectious diseases. Isn't it more useful and more readable to learn "probably caused by an infectious disease" than to hear "probably caused by an infectious disease, and here are the names of nine hundred infectious diseases in alphabetical order"? WhatamIdoing (talk) 21:26, 24 February 2010 (UTC)
- I agree with this emerging consensus that a giant list of causes is useless. It makes more sense to list in the parent article several of the major causes of (insert symptom here), and then supply external links that go into more detail. PDCook (talk) 21:30, 24 February 2010 (UTC)
So, my lists are in no danger of deletion? Immunize (talk) 21:52, 24 February 2010 (UTC)
- No, the consensus seems to be that these lists are not encyclopedic. I agree with that consensus. The useful parts of these lists should be merged into the parent articles. Eubulides (talk) 21:56, 24 February 2010 (UTC)
- I would like to add to PdCooks comment that a brief summary of each condition listed in the differential would put the condition into context and add greatly to the article.Doc James (talk · contribs · email) 22:01, 24 February 2010 (UTC)
There seems to be consensus that these lists are not useful. What should we do with them? Can we identify them here? I can merge some of the smaller ones, but some of the list articles are quite large and I wouldn't know where to start. I should mention that User:Immunize is still generating these lists, such as List of causes of fatigue and List of causes of emesis. PDCook (talk) 23:48, 28 February 2010 (UTC)
It is very difficult to compile thorough differential diagnosis lists. The best ones tend to be found in review articles and texts written by expert practitioners. I just did a quick review of DiagnosisPro and tested several problems with which i have some expertise: growth failure, hypoglycemia in infancy, adrenal failure, and ambiguous genitalia. It failed even to mention some major causes in a routine differential for each of the problems, leaving out whole categories of disease. I would not even recommend it as a starting point for a medical student. We should not be linking anything to it.
Despite the obvious effort put into them, User:Immunize's lists are similarly challenged. The two I checked are so incomplete as to be fairly useless. The two I just looked at (fatigue and emesis) feature exotic problems rarely seen for the last 25 years (e.g. Reye syndrome) while missing common ones (e.g. eating disorders). Anyone with expertise can look at those lists and immediately think of several important conditions omitted, while anyone without expertise has no way to guess how incomplete the lists are. Without some system for trying to achieve at least completeness of the major causes, it's hard to imagine who might benefit from partial lists. There is no way to say this without seeming to deprecate user:Immunize's efforts, but I agree with JFW that without article context and interpretive guidance, the lists themselves have little value here. alteripse (talk) 21:14, 1 March 2010 (UTC)
- Many of diagnosis pro's differentials have over 1000 items listed as differentials. I think this only just emphasis the difficult of generating such lists. The people who started diagnosis pro are not pediatricians so some of the missed content is understandable. Does anyone have a better source of differentials? I think we should link to something and not attempt to generate them here.Doc James (talk · contribs · email) 21:55, 1 March 2010 (UTC)
- The DiagnosisPro lists for ambiguous genitalia, hypoglycemia in infancy, and growth failure are not adult problems are they? They are so bad I would reject them from an intern: they look left over from 1975, and I promise all three differential diagnosis lists have changed immensely from that decade. I only looked at 4 topics but all were poor-- can you point me to any of their lists that actually include all major (not rare) diagnoses? alteripse (talk) 02:52, 2 March 2010 (UTC)
- Many of diagnosis pro's differentials have over 1000 items listed as differentials. I think this only just emphasis the difficult of generating such lists. The people who started diagnosis pro are not pediatricians so some of the missed content is understandable. Does anyone have a better source of differentials? I think we should link to something and not attempt to generate them here.Doc James (talk · contribs · email) 21:55, 1 March 2010 (UTC)
- That's exactly the point, James. If Alteripse can find pages that are rubbish, and you can find pages that "ain't bad" there is a serious inconsistency in the quality of DiagnosisPro which badly affects its reliability. The "about" page states that physicians update it from high-quality sources, but the process is vague, the criteria are undefined, the physicians are anonymous (another page lists three)... Why should we rely on this if we can use textbooks (Harrison's, for instance), peer-reviewed secondary sources, and such? JFW | T@lk 09:37, 2 March 2010 (UTC)
- I am only suggested that sometimes we add a link within the template:infobox symptom when the differential provided is good. I am not suggesting we use this as a reference to generate lists of differentials. I do not think such lists are a good idea here on Wikipedia. BTW if you email them they will update the list with suggestion / sources provided.Doc James (talk · contribs · email) 09:41, 2 March 2010 (UTC)
- The problem with linking to Harrison's is that most people do not have easy access.Doc James (talk · contribs · email) 22:04, 2 March 2010 (UTC)
- Perhaps if we believe a given page at this website to be reasonably complete, then it could be listed as a plain old External link in an appropriate article. This avoids institutionalizing any single website as "the" source in a template; it would be simple to exclude specific pages identified as inadequate; it would be easy to switch to a different website if a better one were found. Furthermore, it's a well-understood, low-overhead and anti-bureaucratic process. Perhaps if we do this for a while, we'll be able to figure out what might be best in the long-term. WhatamIdoing (talk) 01:35, 3 March 2010 (UTC)
Update
Update - I have listed the "diarrhoea" and "fever" lists for AFD. If these both lead to deletion decisions then we have a precedent for eliminating the others. Can I remind Immunize to stick carefully to WP:MEDMOS and WP:MEDRS? You are free to observe the process by which experienced editors produce reliable medical content, and emulate their approaches. JFW | T@lk 08:46, 2 March 2010 (UTC)
Would a move of my lists to the article incubator for improvement be reasonable? Immunize (talk) 20:55, 3 March 2010 (UTC)
- I think that would be fair. If each of the different conditions were expanded into a short summary discussing how frequently it causes said symptom / sign and than listed in most common to least common I would support its integration into the main article / continued existence of the list.Doc James (talk · contribs · email) 21:13, 3 March 2010 (UTC)
Update Per AfD discussion, List of causes of fever and List of causes of diarrhea have been deleted. However, several other list articles remain. Personally, I favor improving the articles rather than nominating them for deletion. Immunize (talk) 16:10, 11 March 2010 (UTC)
Also, I could move the remaining lists to my userspace for improvement, and then move them back into the article space. Immunize (talk) 16:16, 11 March 2010 (UTC)
- You can always copy and paste articles into your own userspace to work on them if they are not deleted. Articles which have been deleted can be restored to user space by an admin willing to do that - there's a list here: Category:Wikipedia administrators who will provide copies of deleted articles and we have an article giving tips on using your user space here: Wikipedia:Userfication. Hope that helps --RexxS (talk) 17:26, 11 March 2010 (UTC)
- Yes drop me a note when you have improved these lists and will be happy toke a look at them. Doc James (talk · contribs · email) 17:40, 11 March 2010 (UTC)
In what way should the pages be improved-do you think it would be appropriate to add an "other symptoms" section to put the illness into context-for instance, in the case of meningococcemia, saying:Other symptoms of meningococcal meningitis include petechiae and purpura, emesis, severe headache, and meningismus. P.S. You suggested a copy and pastemove of the remaining lists into my userspace, but as far as I know copy and paste moves are not advised. Immunize (talk) 20:55, 11 March 2010 (UTC)
- I suggest that you carefully consider the results of the AfD discussions. Even hundreds of hours' efforts might not be capable of sufficiently improving some articles. For one thing, you've got to start with a notable topic, no matter what. For another, the list has to make sense for an encyclopedia. Most lists of non-specific symptoms won't do that.
- In terms of providing context, I think that the most useful thing would be a set of sources that would allow you to indicate relative prevalence of associated conditions. If a symptom's cause is 99% infectious disease, and 1% genetic, then you don't want readers to leave the list thinking that infection and genetic causes are equally likely. Doing this will cut down on the incidence of medical student syndrome and accidental zebra-chasing among our readers.
- Jmh649 is probably not suggesting that you use copy-and-paste to move the page out of the mainspace to work on it; I think he's suggesting that you leave the mainspace copy where it is, and put an entirely separate copy in your userspace to work on it. WhatamIdoing (talk) 21:06, 11 March 2010 (UTC)
- Yes thanks for clarifying that. Please look at the differential diagnosis section of testicular pain [6] for what I am suggesting.Doc James (talk · contribs · email) 15:26, 12 March 2010 (UTC)
I would think that, if the articles are changed to something more similar to what you showed me at Testicular pain, they would need to be moved to a title such as Causes of fever, as they would no longer be in list format. Immunize (talk) 14:00, 13 March 2010 (UTC)
- Yes agree. I do not feel that a list is useful for this type of information. And yes if these are expanded they should be moved to Differential diagnosis for a fever. Doc James (talk · contribs · email) 14:10, 13 March 2010 (UTC)
Yes, I agree that this would be the title for the articles in question. Immunize (talk) 14:39, 13 March 2010 (UTC)
![]() Done I have moved my userspace copy of List of causes of fever to the title you suggested. Should I move the lists still in the article space to this title as well? Immunize (talk) 15:37, 13 March 2010 (UTC)
Done I have moved my userspace copy of List of causes of fever to the title you suggested. Should I move the lists still in the article space to this title as well? Immunize (talk) 15:37, 13 March 2010 (UTC)
- I wouldn't bother -- at this time. The others are still lists at the moment, after all. WhatamIdoing (talk) 18:16, 13 March 2010 (UTC)
Working in userspace
Would you recommend me moving the remainder of the lists to my userspace? Immunize (talk) 18:33, 13 March 2010 (UTC)
- Yes would think that would be a good idea.Doc James (talk · contribs · email) 20:47, 13 March 2010 (UTC)
![]() Done I have moved all of the lists to my userspace for improvement. Also, I added Ewing's sarcoma to User:Immunize/Differential diagnosis for a fever, and have included a short description of the disease itself. Immunize (talk) 21:02, 13 March 2010 (UTC)
Done I have moved all of the lists to my userspace for improvement. Also, I added Ewing's sarcoma to User:Immunize/Differential diagnosis for a fever, and have included a short description of the disease itself. Immunize (talk) 21:02, 13 March 2010 (UTC)
Would it be acceptable to copy and paste information from another Wikipedia article (for instance, in the case of Ewings sarcoma) and use that to create a short summary? Immunize (talk) 13:57, 16 March 2010 (UTC)
- What do you mean by "another Wikipedia"? WhatamIdoing (talk) 04:10, 17 March 2010 (UTC)
I mean another Wikipedia article. Immunize (talk) 14:15, 17 March 2010 (UTC)
- If another wiki releases its content under a compatible licence, then we are free to use that content here, as long as it is correctly attributed (a detailed note in the edit summary is generally considered sufficient). However, we must still comply with our sourcing policies. A wiki is not a reliable source (other than for its opinions about itself), so any content imported would still have to have external sources that meet WP:MEDRS in the case of medical articles. --RexxS (talk) 04:32, 17 March 2010 (UTC)
When I say "another wikipedia" I mean another Wikipedia article. Immunize (talk) 14:15, 17 March 2010 (UTC)
- Yes, you can copy information from an article, such as Ewings sarcoma, to use as a summary in another article, such as a list. This is a common behavior when WP:SPLITting articles, although WP:LEAD recommends some thoughtful copyediting. WhatamIdoing (talk) 18:18, 18 March 2010 (UTC)
I have copied and pasted information from Wikipedia into the article User:Immunize/Differential diagnosis for a fever, and have also created subsections for each disease in the article. Immunize (talk) 15:05, 19 March 2010 (UTC)
- That's fine. Just remember to always indicate the source of your copy-paste in your edit summary. It means that anyone can trace back via the source article history who the original contributors were. That has normally been taken to satisfy the licence requirement that all contributions are attributed when re-used. --RexxS (talk) 17:45, 19 March 2010 (UTC)
So I should reference the copy-pasted information? Immunize (talk) 18:35, 19 March 2010 (UTC)
- Sorry if I wasn't clear enough. If you mean adding citations to material to meet WP:V, then yes, of course. But I was talking about our licence which requires wikipedia material to be attributed (not the same thing as a citation) to the original author when it is re-used. When you add material to an article, you are effectively claiming authorship of what you contribute, unless you make a disclaimer in the edit summary that you are copying someone else's work (which is released under a CC-BY-SA licence). If you summarise, then it's your work and requires nothing more than the usual citations. If you copy near-verbatim from another wikipedia article, then it's best practice to make a note in your edit summary where you took the text from. Hope that is clearer now. --RexxS (talk) 03:52, 20 March 2010 (UTC)
It is verbatim from Wikipedia, because it is a direct copy-paste from a Wikipedia article. So you are saying I should cite it as from wikipedia and note in the edit summary that it is copy-pasted from Wikipedia, right? Immunize (talk) 14:15, 20 March 2010 (UTC)
- You just need to state in the edit summary that it is from [[so and so a page]] Doc James (talk · contribs · email) 14:49, 20 March 2010 (UTC)
I have improved the article User:Immunize/Differential diagnosis for a fever significantly over the past several days, and feel it may soon be time to move it back into the article space. Can an experienced medical wikipedian please look at it and give me their opinion? Immunize (talk) 19:54, 23 March 2010 (UTC)
Why has there been no response? I have edited the User:Immunize/Differential diagnosis for a fever article significantly, and it is now ready for review and possible move back to the article space. Immunize (talk) 18:58, 3 April 2010 (UTC)
- Immunize, I respect the effort that you put in to improve the quality of this list. However Wikipedia is not intended to be a manual or textbook. Indeed apart from the referencing, I don't see that your new version of the list is any better than previous versions. I don't see how this list is useful and I don't think that it has a place in Wikipedia. Axl ¤ [Talk] 19:23, 6 April 2010 (UTC)
Are there any other measures I could take to improve the list? Immunize (talk) 22:08, 7 April 2010 (UTC)
- As you know, the differential diagnosis for a fever is huge. I don't think that putting all of this information into one article is helpful. This is not the purpose of an encyclopedia. Axl ¤ [Talk] 07:48, 10 April 2010 (UTC)
Would it be more appropriate to split the article into smaller articles such as "infectious causes for fever" or "neoplastic causes for fever"? Immunize (talk) 12:48, 10 April 2010 (UTC)
- I have posted comments here User_talk:Immunize/Differential_diagnosis_for_a_fever Doc James (talk · contribs · email) 16:50, 10 April 2010 (UTC)
So, as I understand it, you feel that this article is still a list despite the addition of large amounts of text in an attempt to put the list into context? Immunize (talk) 16:53, 10 April 2010 (UTC)
I suppose I am starting to doubt that these lists will ever be improved beyond there current state, given that you do not feel that, even after at least a month of work the lists are still not ready for move to the article space. Immunize (talk) 19:03, 18 April 2010 (UTC)
- In my opinion, the quality of this article is much improved. However I'm still not convinced that it should be in Wikipedia. I await the views of other WikiProject Medicine editors. Axl ¤ [Talk] 19:44, 20 April 2010 (UTC)
- I think the article needs much working and copy-editing before being ready to move to the main space, and the article have no standers, I mean there is some expansion on some diseases, and there is a little about other, it needs more working MaenK.A.Talk 21:11, 20 April 2010 (UTC)
- Before I would be happy to see this go back to the main space I wish to see the relative importance of the different causes conveyed. Otherwise this is little more than just a list of causes which is of questionable encyclopedic content as the potential list can reach to thousands.Doc James (talk · contribs · email) 22:24, 20 April 2010 (UTC)
- To user madhero88:Please specify what improvement you feel that the list needs prior to a move back to the article space. Immunize (talk) 20:26, 21 April 2010 (UTC)
- I am becoming somewhat exasperated with the lack of response after at least a week of waiting for a reply. I currently do not know what to do with these lists; however I am considering splitting them into several subarticles, as currently the list is so long (200+ kilobytes) that I am having technical difficulties editing it. Immunize (talk) 16:28, 28 April 2010 (UTC)
- UpdateI have split the "infectious" section into the article User:Immunize/Infectious causes for a fever.
- I am now splitting the User:Immunize/Differential diagnosis for a fever article into multiple smaller articles. My plan is that I will improve the smaller articles, and then copy-paste the improved text back into the main article ( User:Immunize/Differential diagnosis for a fever ). I will then (after consensus that these list is ready for the article space) move the main article ( User:Immunize/Differential diagnosis for a fever ) back into the article space. Best wishes. Immunize (talk) 18:11, 8 May 2010 (UTC)
- UpdateI have split the "infectious" section into the article User:Immunize/Infectious causes for a fever.
- I am becoming somewhat exasperated with the lack of response after at least a week of waiting for a reply. I currently do not know what to do with these lists; however I am considering splitting them into several subarticles, as currently the list is so long (200+ kilobytes) that I am having technical difficulties editing it. Immunize (talk) 16:28, 28 April 2010 (UTC)
- To user madhero88:Please specify what improvement you feel that the list needs prior to a move back to the article space. Immunize (talk) 20:26, 21 April 2010 (UTC)
Convulsion and seizure same thing
I was under the impression that a seizure and convulsion are the same thing but we have two seperate articles with the same ICD9 and Mesh codes. I think that they need merged, but I am open to persuasion. :)--Literaturegeek | T@1k? 19:02, 22 April 2010 (UTC)
- We also have Non-epileptic seizure and Psychogenic non-epileptic seizures as well, so seizure probably needs to be considered a rather broader term than convulsion. I'm also willing to be persuaded, but I think that convulsion is specifically characterised by muscle spasms, and seizure (while encompassing that) can occur without that symptom (as in Absence seizure). Take that for what it's worth, as I'm just Joe Public, not a medical practitioner. --RexxS (talk) 19:41, 22 April 2010 (UTC)
- I think that they should be merged as they are essentially the same think. Non epileptic seizures and psychogenic seizure are subtypes of seizure however convulsions is just a laymen term for seizures. I looks at the classification system Seizure types and it does not appear to mention convulsions.--Doc James (talk · contribs · email) 20:37, 22 April 2010 (UTC)
Both our seizure and seizure types articles deal solely with epileptic seizures. The reason they are at seizure and not epileptic seizure is our WP:COMMONNAME policy. There is an argument that they should be at the full unambiguous name and that seizure should be a DAB. However, that would require fixing many links and break WP:COMMONNAME. This is the problem we have that accurate naming conflicting with WP policy. The proposed mergers don't help without fixing the above accurate naming issues.
A convulsion is a muscle spasm and when the cause is epileptic, the precise term would be a clonic seizure, which is listed in seizure types, and this can occur as a phase within a tonic-clonic seizure that many people are familiar with. An older term was grand mal seizure. But convulsions can have non-epileptic causes. There are many non-convulsive epileptic seizure types, though many people (including medics) are unfamiliar with them. The word "convulsion" isn't just a lay term: it accurately describes the visible manifestation that the patient or an observer saw.
The term seizure is imprecise but when used by medics is nearly always an abbreviated way of saying "epileptic seizure". A medic wouldn't describe a heart attack as a seizure or a fit of rage as a seizure. The word "fit" also has a broad range of uses, and is used by both lay and medics as a word for epileptic seizures too.
Non-epileptic seizures (of which psychogenic seizures are one kind) are a different kettle of fish. Some might argue they are simply a classification of misdiagnoses rather than a disorder someone should be diagnosed with. For example, someone might be suspected of having seizures but it turns out they are having fainting fits. They don't belong in the ILAE classification of (epileptic) seizures. To say they are a "subtype" of seizure is wrong in much the same way as a classification of animals doesn't have "stuffed toy" as a subtype, even though "teddy bear" shares the same word and has some similarities with a "bear". Colin°Talk 22:00, 22 April 2010 (UTC)
- It may be helpful to remember that WP:COMMONNAME allows many specific exceptions and WP:MEDMOS#Naming conventions is an important one. The argument, in brief, is that COMMONNAME is a default position where no other considerations overrule it. In the case of medicine-related articles, universally recognised naming and classification schemes exist and it makes sense to use those, rather than try to reach a consensus on what is the commonest name used in English. Redirects will always take care of the synonyms. Since it seems our Seizure article deals almost exclusively with epileptic seizures, I'm attracted to the idea of renaming it to Epileptic seizure and creating a dab page at Seizure to replace Seizure (disambiguation). The alternative would be to split off Epileptic seizure and re-write Seizure as a summary article, covering all of our articles that contain the word seizure in the title, as well as Convulsion. I suspect that the latter would be overkill, and that a reader looking for an article on seizures would be as well served by a well-constructed dab page.
- As an aside to Colin, it's also interesting to note that Wikipedia's classification system is not always consistent. Hopkin Green Frog, a stuffed toy, is in Category:Fictional frogs and toads, which is a sub-category of Category:Animals in popular culture, which is a sub-category of Category:Animals. So there's at least one stuffed toy in Animals (although, perversely it's not in Category:Stuffed toys!) <grin> --RexxS (talk) 23:21, 22 April 2010 (UTC)
- Even though I agree convulsions is technically slightly different than seizure I do not think it warrants its own page but could be satisfactorily explained in the definitions section of the seizure article along with pseudoseizures.Doc James (talk · contribs · email) 00:04, 23 April 2010 (UTC)
- Since the Convulsion article is so short, I'm tempted to agree, James. The two problems I can foresee are: (1) that (per WP:MEDMOS#Sections), there is no Definition section, and the lead should contain very little material not covered elsewhere in the article; (2) we should have a section that Convulsion would redirect to. I suppose that the contents of the Convulsion article could be written into the lead of the Seizure article and Convulsion redirected to Seizure, but I'm not sure that improves things for the reader. --RexxS (talk) 00:46, 23 April 2010 (UTC)
- Agree that one good solid article under seizure is the best way forward. Casliber (talk · contribs) 02:44, 23 April 2010 (UTC)
- If you look at the Wikipedia:Manual_of_Style_(medicine-related_articles)#Symptoms_or_signs it does have a section for definitions. I have added definitions as an option to WP:MEDMOS as the classification section is usually a good area to define related terms. If the convulsion section than becomes to big it can be slit off but I think as there is so much overlap between these terms that this will probably not be an issue.Doc James (talk · contribs · email) 03:08, 23 April 2010 (UTC)
- That looks sensible, James. I was looking only at WP:MEDMOS#Diseases or disorders or syndromes as that was where I thought epileptic seizures fitted, and that part of MEDMOS didn't have a definitions section until you just added it. I'd say go ahead with the merge. You might want to use the formal procedure or just drop a notice on the Talk:Convulsion page. --RexxS (talk) 07:15, 23 April 2010 (UTC)
- I'll have a think about convulsion to see if it could be expanded or would remain little more than a dictdef. I'm a bit confused about Casliber's point. What would the "one good solid article" cover? I would be very much opposed to an article (as opposed to a DAB) that mixed epileptic and non-epileptic "seizures": this is never ever done in the literature and would confuse the readers. Again, this would be like animal having paragraphs on the stuffed variety. Colin°Talk 08:02, 23 April 2010 (UTC)
- That looks sensible, James. I was looking only at WP:MEDMOS#Diseases or disorders or syndromes as that was where I thought epileptic seizures fitted, and that part of MEDMOS didn't have a definitions section until you just added it. I'd say go ahead with the merge. You might want to use the formal procedure or just drop a notice on the Talk:Convulsion page. --RexxS (talk) 07:15, 23 April 2010 (UTC)
- If you look at the Wikipedia:Manual_of_Style_(medicine-related_articles)#Symptoms_or_signs it does have a section for definitions. I have added definitions as an option to WP:MEDMOS as the classification section is usually a good area to define related terms. If the convulsion section than becomes to big it can be slit off but I think as there is so much overlap between these terms that this will probably not be an issue.Doc James (talk · contribs · email) 03:08, 23 April 2010 (UTC)
- Agree that one good solid article under seizure is the best way forward. Casliber (talk · contribs) 02:44, 23 April 2010 (UTC)
- Since the Convulsion article is so short, I'm tempted to agree, James. The two problems I can foresee are: (1) that (per WP:MEDMOS#Sections), there is no Definition section, and the lead should contain very little material not covered elsewhere in the article; (2) we should have a section that Convulsion would redirect to. I suppose that the contents of the Convulsion article could be written into the lead of the Seizure article and Convulsion redirected to Seizure, but I'm not sure that improves things for the reader. --RexxS (talk) 00:46, 23 April 2010 (UTC)
Wrt renaming seizure to epileptic seizure and having Seizure (disambiguation) become seizure. WP:COMMONNAME recognises there are competing arguments for the current situation and the suggested one. Precision is the main reason for using epileptic seizure. But it fails on the recognizable, easy to find, concise and consistent tests. For example, the test for a name "which editors will most naturally link from other articles". The links seizure or seizures are used 1,101 times; the links epileptic seizure and epileptic seizures are used only 281 times. Nearly all of those 1,101 times refer to an epileptic seizure, though in some cases it may be hard to know.
The other test is WP:PRIMARYTOPIC, where we judge whether "epileptic seizure" is what is nearly always meant by the term "seizure". I believe it is. This is reinforced by the article linking stats.
Lastly, our policy requires us to be "guided by the usage in reliable sources". A search on PubMed for article titles, shows that "seizure" or "seizures" are used 21,871 times and "epileptic seizure" or "epileptic seizures" are used only 1,777 times. Again, the articles with "seizure" in the title are almost universally referring to an epileptic seizure.
If this was an non-hyperlinked medical encyclopaedia, I'd probably vote for the article to be epileptic seizure as this is the precise term. But Wikipedia isn't. Colin°Talk 09:13, 23 April 2010 (UTC)
- Another option is to rename seizure to epileptic seizure, keep seizure as a redirect to epileptic seizure, leave seizure (disambiguation) as is, and redirect convulsions to epileptic seizures. A hatnote, such as {{Redirect6|seizure|non-epileptic seizures|Non-epileptic seizure}}, should be added to epileptic seizure, which would say "seizure" redirects here. For non-epileptic seizures, see Non-epileptic seizure. For other uses, see seizure (disambiguation). I like the idea to include the definition of convulsion in the epileptic seizure article. This solution is a way to keep the epileptic seizures under the common name and primary topic of seizures, yet still be medically precise. --Scott Alter 14:13, 23 April 2010 (UTC)
Seizure has quite non-medical meanings as well that will not show on PubMed. A court of law may be "seized of a matter", pirates may "seize a ship", and in tribology poorly-lubricated surfaces in contact may "seize" each other. Any of these kinds of seizure could merit articles of their own, but would seem inappropriate to class as "non-epileptic". Seizure should be a simple disambiguation page with epileptic seizure as the first entry. Other medical meanings might come near the top of that page, but users should not need double redirects to find those other meanings. User:LeadSongDog come howl 15:13, 23 April 2010 (UTC)
- I still believe that "seizure" has a primary use, and it is an epileptic seizure. Therefore, the epileptic seizure article, whatever it may be called, should be what seizure directs to (whether directly located there or as a redirect), and seizure should not be a disambiguation page. WP:DAB mentions that disambiguation is only needed for existing articles - so if there are no articles about the other uses you have mentioned, they do not need to be disambiguated. The fact that articles on these other uses of "seize" further indicates that they are not the primary topic of the word. The hatnote on seizure currently says, This article is about epileptic seizures. For non-epileptic seizures, see Non-epileptic seizure. For other uses, see Seizure (disambiguation)., which is why I recommended using {{redirect6}}. However, if you believe someone might consider "pirates seizing a ship" to be a "non-epileptic seizure," I might consider making the hatnote, "Seizure" redirects here. For other uses, see Seizure (disambiguation). ({{redirect}}). --Scott Alter 15:40, 23 April 2010 (UTC)
- I would be happy with Scott's suggestion.Doc James (talk · contribs · email) 16:00, 23 April 2010 (UTC)
- In the news, it mostly refers to seizures by authorities. See [7]. User:LeadSongDog come howl 16:13, 23 April 2010 (UTC)
- Most of the other uses involve the verb "to seize" but not the noun "seizure". And although "seizure" is used wrt the enforced capture of goods (illegally or legally), it is just a boring word that wouldn't inspire an encyclopaedia article. We aren't a dictionary so don't have to consider all uses of a word to be equal. I think Scott's suggestion could work and I'd certainly be happy with the article being at the precise term and it avoids having over 1000 articles suddenly pointing at a DAB.
- Having looked at most of the wikilinks for convulsion, it seems to be generally be being used as a synonym for a seizure. Drugs can be classified as convulsants and anticonvulsants. So turning this into a redirect to epileptic seizure would seem to fit the WP:PRIMARY usage. I think an admin is required to make the proposed changes. Colin°Talk 17:59, 23 April 2010 (UTC)
- Have a look at search and seizure. Note that it is not search and seize. This present venue is principally of interest to editors of medical articles, so it is not surprising that editors here are focussed on the medical meanings, but the change being discussed impacts, for example, WP:WikiProject Law where the perception may be different. User:LeadSongDog come howl 18:19, 23 April 2010 (UTC)
- In the news, it mostly refers to seizures by authorities. See [7]. User:LeadSongDog come howl 16:13, 23 April 2010 (UTC)
- I also like Scott's suggestion. If desired, the page can be moved to Epileptic seizure if desired to clarify the medical topic under discussion, so long as Seizure remains a redirect to it. Anecdotally, I work with legal matters as my day job, and I feel strongly that the common usage of seizure means epileptic seizure and so shouldn't be turned in to a summary or dab. VernoWhitney (talk) 19:08, 23 April 2010 (UTC)
- I would be happy with Scott's suggestion.Doc James (talk · contribs · email) 16:00, 23 April 2010 (UTC)
I also agree with Scott's suggestion, and would add that an admin isn't needed to move Seizure to Epileptic seizure over the redirect, since the history is trivial. However, when checking that, I noticed the log:
- 15:59, 26 June 2008 Fvasconcellos (talk | contribs) (21 bytes) (moved Epileptic seizure to Seizure: per discussion and WP:NC)
So it seems that we're proposing to reverse a move that had discussion in June 2008 – although I don't see that discussion at Talk:Seizure. --RexxS (talk) 19:09, 23 April 2010 (UTC)
- There's some conversation regarding that and other related moves here. VernoWhitney (talk) 19:23, 23 April 2010 (UTC)
- I found the discussion the move refers to at User talk:Colin/Archive 4#Seizure types. The discussion we are having now is not the reverse of the previous discussion. To summarize, in June 2008, Seizure was moved to Epileptic Seizure, and Seizure was turned into a disambiguation page (currently at Seizure (disambiguation)) without consensus. It was then decided that "epileptic seizures" were the primary use of the word "seizure," and Seizure should not be a disambig page. So the dab page formerly at Seizure was moved to Seizure (disambiguation), and Epileptic seizure was moved back to Seizure. At that time, there was no discussion of making Seizure a redirect. Convulsion was not created as its own article until after this discussion, in September 2008. Also, since it seems like Seizure is going to be renamed, should Seizure types also be renamed, perhaps to Epileptic seizure types (or Types of epileptic seizures, Epileptic seizure classification, or Classification of epileptic seizures)? --Scott Alter 19:26, 23 April 2010 (UTC)
- I thought we had discussed this all before, glad you found the link to remind me. Note the situation at June 2008 was a result undiscussed changes by Tatterfly. I think Fvasconcellos mostly moved things back to how they always had been, with the exception that convulsion became an article rather than the redirect to seizure that it was. So I think the above commentary just confuses things by describing a temporary and broken situation. The last time, we nearly went for something close to the option suggested by Stott but chickened out and just reverted back to how it was. Although there are WP:NC arguments for using the shortened for seizure as the main article, there are also WP:NC arguments for using the precise term provided the shortened form (the common form) doesn't become a DAB. I don't know if there are any double-redirect problems with making seizure are redirect: perhaps they need fixed too. I think the case for moving seizure types is less strong as we should favour the concise term unless there are good reasons. Colin°Talk 20:28, 23 April 2010 (UTC)
- I found the discussion the move refers to at User talk:Colin/Archive 4#Seizure types. The discussion we are having now is not the reverse of the previous discussion. To summarize, in June 2008, Seizure was moved to Epileptic Seizure, and Seizure was turned into a disambiguation page (currently at Seizure (disambiguation)) without consensus. It was then decided that "epileptic seizures" were the primary use of the word "seizure," and Seizure should not be a disambig page. So the dab page formerly at Seizure was moved to Seizure (disambiguation), and Epileptic seizure was moved back to Seizure. At that time, there was no discussion of making Seizure a redirect. Convulsion was not created as its own article until after this discussion, in September 2008. Also, since it seems like Seizure is going to be renamed, should Seizure types also be renamed, perhaps to Epileptic seizure types (or Types of epileptic seizures, Epileptic seizure classification, or Classification of epileptic seizures)? --Scott Alter 19:26, 23 April 2010 (UTC)
- Thanks very much for finding the previous discussion. That makes things much clearer now, as we don't need to worry about a previous consensus on the actual article name. Since Seizure is at present in the scope only of WikiProject Medicine, it seems clear to me that WP:MEDMOS#Naming conventions is the principal guidance to follow. The current article is wholly about epileptic seizure and that should be the name of the article. I understand that it's not quite as clear-cut as the situation with Heart attack and Myocardial infarction, but I think the principle remains, as well as satisfying a desire that article titles be precise and unambiguous as far as possible. As the primary use of the word, Seizure should redirect to Epileptic seizure with the {{redirect6}} hatnote that Scott suggests. For me it's important to retain the link to Non-epileptic seizure (which does need improvement), as I'm more normally concerned with seizures resulting from CNS Oxygen toxicity, which I don't think meet the definition of epileptic, but are a concrete example of a seizure as a symptom of another condition. — Preceding unsigned comment added by RexxS (talk • contribs) 21:44, 23 April 2010 (UTC)
- Just for the record: seizure is the accepted medical term for an epileptic seizure (witness the 20,000 usages in journal article titles on Pubmed, and in fact there is a journal called "Seizure"). So this isn't really a MEDMOS vs NC argument. It is more about deciding which of the various conflicting WP:NC qualities we should favour (precision over conciseness, etc). I'm going to post a notice on the seizure article pointing to this debate. Colin°Talk 09:11, 24 April 2010 (UTC)
- I can't figure out what template to add to seizure to point to this discussion. Anyone help? Colin°Talk 09:37, 24 April 2010 (UTC)
- Just for the record: seizure is the accepted medical term for an epileptic seizure (witness the 20,000 usages in journal article titles on Pubmed, and in fact there is a journal called "Seizure"). So this isn't really a MEDMOS vs NC argument. It is more about deciding which of the various conflicting WP:NC qualities we should favour (precision over conciseness, etc). I'm going to post a notice on the seizure article pointing to this debate. Colin°Talk 09:11, 24 April 2010 (UTC)
- I've simply posted a notice linking to this section at Talk:Seizure#Suggested move to Epileptic seizure. If we need to make a move request, then that section can be referred to in the template requesting the move, and will serve as a permanent marker in the article history to our debate. I'm happy to defer to you in the argument that seizure is an accepted medical term, but would then suggest that – because an article covering all uses of seizure as a medical term would be impossibly huge – we should be up-front and call the present article 'Epileptic seizure' as that is precisely its subject. --RexxS (talk) 12:07, 24 April 2010 (UTC)
- Another just-for-the-record: not all seizures are convulsions (e.g. absence seizures, complex partial seizures, atonic seizures). Colin alluded to this at the start of the discussion and of course it's made clear in the articles, but I thought it was worth mentioning explicitly here. Neurotip (talk) 19:23, 24 April 2010 (UTC)
- I thought I mentioned that explicitly in the second comment of this discussion. Before we wind this up by repeating ourselves further, can I just ask if the implication in Convulsion that convulsions can occur without seizure is also true? The article mentions electric shock, but there's no source to back any of that up. The article Electric shock doesn't mention convulsions, other than stating that the objective of the Electroconvulsive therapy is to induce a seizure. The ECT article is rather more explicit in stating that it induces a clonic seizure, but doesn't back that up with a source. I would be nice to find a reliable medical source that clearly states the relationship between seizure and convulsion. --RexxS (talk) 20:53, 24 April 2010 (UTC)
- The principle difference is that a convulsion is an observable symptom that anyone from parent to neurologist can use to describe what occurred. An epileptic seizure says something about the cause (though doesn't on its own imply epilepsy). Unless an EEG is being taken and the results of the EEG interpreted by an expert, it can sometimes be hard to determine whether an event was really an epileptic seizure. Psychogenic non-epileptic seizures can include convulsions that mimic seizures. Electricity could cause a seizure but can also make a frog's legs twitch. Dorling's medical dictionary mentions a "tetanic convulsion" which seems to have no neurological aspect. Colin°Talk 22:23, 24 April 2010 (UTC)
- Ah, I did not realise that I would have kicked off such a debate. :) I have been convinced that there is indeed a difference between convulsion and seizure, despite that they are commonly used interchangably. Hopefully a sensible agreement can be reached or consensus. Perhaps what is needed is a vote to gather people's views together more clearly.--Literaturegeek | T@1k? 21:32, 24 April 2010 (UTC)
- I thought I mentioned that explicitly in the second comment of this discussion. Before we wind this up by repeating ourselves further, can I just ask if the implication in Convulsion that convulsions can occur without seizure is also true? The article mentions electric shock, but there's no source to back any of that up. The article Electric shock doesn't mention convulsions, other than stating that the objective of the Electroconvulsive therapy is to induce a seizure. The ECT article is rather more explicit in stating that it induces a clonic seizure, but doesn't back that up with a source. I would be nice to find a reliable medical source that clearly states the relationship between seizure and convulsion. --RexxS (talk) 20:53, 24 April 2010 (UTC)
Just a quick note – before this gets archived – that Scott has now kindly done the work of moving Seizure to Epileptic seizure and used {{Redirect6}} to make a sensible hatnote. Hopefully, this will stick and should then reflect much of the consensus here (in case editors want to refer to it in the future). --RexxS (talk) 23:37, 4 May 2010 (UTC)
- To reiterate, I only moved Seizure to Epileptic seizure, as there seemed to be consensus for that move. I did not touch Convulsion, but something should probably still be done between it and Epileptic seizure. --Scott Alter (talk) 02:07, 5 May 2010 (UTC)
- To add to convulsion we also have fasciculation, twitch, and tremor. Do we need all these terms separate Doc James (talk · contribs · email) 03:23, 5 May 2010 (UTC)
- What would you merge to? How would that be better? Colin°Talk 08:06, 5 May 2010 (UTC)
- Have added the term to the main twitch page. A convulsion is twitching. Wondering if we should add seizures too?Doc James (talk · contribs · email) 08:50, 5 May 2010 (UTC)
- What would you merge to? How would that be better? Colin°Talk 08:06, 5 May 2010 (UTC)
- To add to convulsion we also have fasciculation, twitch, and tremor. Do we need all these terms separate Doc James (talk · contribs · email) 03:23, 5 May 2010 (UTC)
Category:Genetic disorders
While working on categorization of diseases, I have come across many articles that are categorized into Category:Genetic disorders and a type of heredity subcategory (such as Category:Autosomal recessive disorders). Is it necessary to put articles in both of these categories? For diseases with known inheritance patterns, I do not think they need to be in the overly generalized Category:Genetic disorders. After all, almost all diseases can be said to have a genetic component. Therefore, I would like to clean up and diffuse Category:Genetic disorders into subcategories based on things like involved chromosomes and dominance. --Scott Alter 15:45, 24 April 2010 (UTC)
- Could you also create a subcategory for genetic disorders with no OMIM code? --Arcadian (talk) 16:43, 24 April 2010 (UTC)
- More specific categorisation is good, there's allways List of genetic disorders if someone wants to find them all in one place! Lee∴V (talk • contribs) 21:43, 26 April 2010 (UTC)
- I'm currently not going through Category:Genetic disorders directly, rather coming across diseases in other categories that are also in Category:Genetic disorders. Are you referring to diseases with no OMIM code or articles lacking the information? In either case, there should be a better way to find genetic disorders without OMIM codes...like maybe having a bot going through all of the articles within Category:Genetic disorders (and 1 sublevel) and create a list. Another option (which I don't think is possible) would be to use {{Infobox disease}} to categorize articles with no OMIM code but are in Category:Genetic disorders. I'm just hesitant to manually categorize articles on this basis. Perhaps we can do something similar to the categorization of drugs without ATC codes (see Template:Drugbox#ATC, ATCvet and CAS, Category:Drugboxes with an unspecified ATC code, and Category:Drugs not assigned an ATC code). Maybe this should be done for other codes (such as ICD) as well. --Scott Alter (talk) 19:46, 4 May 2010 (UTC)
Microscopy illustration
Since microscopy is within your scope, I'm letting you know about this figure that I composed (from previously existing material) that might be useful for illustrating aspects of light and/or electron microscopy. If you need to make changes that will reduce the EV in the three butterfly-related articles where it's currently placed, please create a fork instead. Thank you.
Photographic and light microscopic images 

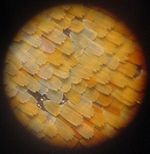
Zoomed-out view of an Aglais io. Closeup of the scales of the same specimen. High magnification of the coloured scales (probably a different species). Electron microscopic images 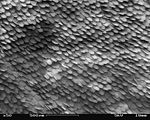


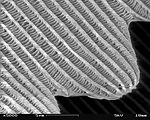
A patch of wing Scales close up A single scale Microstructure of a scale Magnification Approx. ×50 Approx. ×200 ×1000 ×5000







Papa Lima Whiskey (talk) 11:38, 1 May 2010 (UTC)
- Those images look amazing. ---kilbad (talk) 15:14, 1 May 2010 (UTC)
- Wow. This is fascinating. I feel like I did when I was a little kid at the science museum! Great job! TypicalUser (talk) 15:31, 4 May 2010 (UTC)
UpToDate use or overuse
I raised a query re use of this subscription only source at WT:MEDRS, initial reponse suggested here might have been a better location for the query - see WT:MEDRS#Use or overuse of UpToDate. David Ruben Talk 23:08, 1 May 2010 (UTC)
- Use of a source that one cannot access at a major university library should be discouraged IMO. One should either use the source that Uptodate quotes or verify the content in more accessible literature. I BTW do love Uptodate and this is what I base my practice on but the cost of $1000 USD for three years is to much for most of the world.Doc James (talk · contribs · email) 23:13, 1 May 2010 (UTC)
- Although UpToDate is a subscription source, that does not affect the consideration of whether it's a reliable source. The requirement of verifiability is that someone (not necessarily everyone) can check the source to see if it verifies the claim made (see WP:PAYWALL).
- Looking at WP:RS#Overview, the opening sentence is "Articles should be based on reliable, third-party, published sources with a reputation for fact-checking and accuracy." I believe that UpToDate is independent and peer-reviewed, but further research would need to be done to establish if it has a reputation for fact-checking and accuracy. If so, then it's clearly a reliable source for the purposes of Wikipedia. The only question then left is whether it should be considered as a secondary or tertiary source, and that may well depend on the nature of its own sources, so I guess that would have to be considered on a case-by-case basis.
- In the case of the refs inserted in Graves disease, perhaps we could ask Doc James to have a look when he has a moment to spare? I'd be willing to trust his judgement on how well the refs support the text made there. --RexxS (talk) 00:36, 2 May 2010 (UTC)
- I am able to give out one time one month memberships to Uptodate. I am also allowed to forward single topics to people. If someone wishes one to go over these edits I would be happy to send access to Uptodate. All I need is an email address.Doc James (talk · contribs · email) 01:26, 2 May 2010 (UTC)
I have never regarded UpToDate as a useful source for Wikipedia. It is a continuously-changing professional resource, much like Emedicine articles, and is clearly intended to be a practical resource. In contrast, high-quality journal reviews do not change until they are updated and are clearly more suitable. Having skimmed a fair number of UpToDate articles, I'm also struck by the fact that its authors sometimes get really obscure. On the whole, UpToDate entries are not equivalent to journal reviews and should be avoided. JFW | T@lk 07:29, 2 May 2010 (UTC)
- That's a very sensible point, JFW, and I think it translates in Wikipedia terms into treating UpToDate more as a tertiary source than as a secondary. The question I think David raises is how to respond to an editor who relies on a lot of UpToDate citations. Perhaps we could agree that we can recognise UpToDate as a starting point for finding sources, but we ought to discourage editors from relying on just the UpToDate source for medical claims? --RexxS (talk) 11:44, 2 May 2010 (UTC)
- I'm inclined to agree with JFW as well - Uptodate might be a great place to mine for sources, but not necessarily a great place to draw from directly. Pity it's a paywall site, because it could certainly be useful for infoboxes, like eMedicine... WLU (t) (c) Wikipedia's rules:simple/complex 13:30, 2 May 2010 (UTC)
UpToDate is certainly one of the best online resources for clinical care in the US. It is expensive and most of us rely on hospital or university access. It is typically more comprehensive and less uneven than Emedicine, with better details of treatment. While UpToDate is fairly well referenced, I agree w JFW that it is not a reference of choice for WP because of the expensive cost of access and frequent revisions, but also because to this point there is nothing in it for which there is not a standard reference. {Parenthetically I am always surprised and slightly disturbed at how many house officers will openly admit they start with WP, since UpToDate has a considerably burdensome log-in threshold). alteripse (talk) 17:39, 2 May 2010 (UTC)
- I agree with the above and would support a statement from WP:MED saying that Uptodate should not be used to reference content on Wikipedia due to issue of access and the fact that the content changes over time. Emedicine is easier to access but I do not view it as the best source either. We should really emphasize that the majority of references should be to either: 1) journals, 2) textbooks, 3) government publications Doc James (talk · contribs · email) 18:41, 2 May 2010 (UTC)
- I think that 'banning' or even 'dis-recommending' UpToDate is a bad idea. I'd choose UpToDate over nearly any patient-oriented website, and even over a stack of primary sources. Telling someone, "Thanks for all of your work in providing accurate and properly sourced information, but we think you're using a second-best source, so please stop it" -- when we have thousands of articles with truly lousy sources -- is IMO a poor use of our energy and a lousy way of thanking someone for their clearly positive efforts.
- The fact that it is behind a paywall is absolutely irrelevant: A lot of top-quality journal articles are equally hidden behind paywalls. It's silly to reject UpToDate, at $40 a month, on the grounds of cost while approving, in the same sentence, of journals that charge $40 per article, or medical textbooks and reference works at $400 each.
- The fact that UpToDate changes is (or could be) an issue, albeit an issue that applies to thousands of online sources. The
|accessdate=parameter is designed for exactly that situation. - The bottom line is that while I think we can encourage the use of academic sources, we should not reject, or even discourage, use of good sources like UpToDate. We don't need the best to be the enemy of the good here, especially when the battle with truly dreadful sources is still underway. WhatamIdoing (talk) 00:56, 4 May 2010 (UTC)
- I agree with WAID above. UpToDate appears to provide reliable information which is actually used by practising professionals: in my mind, that puts it on a line with textbooks. The fact that it gets updated more often than most textbooks should hardly be a barrier to its use: we can find a way to cite a particular version. Access costs shouldn't be an issue either: most Wikipedia users don't have access to medical textbooks or UpToDate, that's precisely why they use WP! Physchim62 (talk) 01:08, 4 May 2010 (UTC)
- I must say that I agree that it is better than
bothvertically all websites. It is definitely reliable however well one can get access to journals at most University libraries Uptodate can be harder to access. So I would say that review articles published in journals are preferred. Uptodate is in line with textbooks.Doc James (talk · contribs · email) 01:54, 4 May 2010 (UTC)
- I must say that I agree that it is better than
- I agree with WAID above. UpToDate appears to provide reliable information which is actually used by practising professionals: in my mind, that puts it on a line with textbooks. The fact that it gets updated more often than most textbooks should hardly be a barrier to its use: we can find a way to cite a particular version. Access costs shouldn't be an issue either: most Wikipedia users don't have access to medical textbooks or UpToDate, that's precisely why they use WP! Physchim62 (talk) 01:08, 4 May 2010 (UTC)
I have never thought of it as a "patient oriented website". I would not dispute that it is an excellent site for practicing physicians who have access to it. That said, abstracts of standard journal articles are still far more accessible to those who simply want the gist of a reference or to verify that the reference says what the referencer claims it does. While buying single journal articles is prohibitively expensive, there are greater chances of access to many clinical journals at local hospital and university libraries than to UpToDate for most of our readers. Finally, for many purposes, if you have a choice of references the original citation, the most authoritative citation, or the most accessible citation might be preferred, and those three criteria are still not likely ever to be UpToDate. alteripse (talk) 02:33, 4 May 2010 (UTC)
- I agree with Doc and JFW that it should be discouraged. While perhaps it couldn't be technically prohibited under MEDRS, it can certainly be discouraged, and there's nothing preventing us from replacing it or asking the editor to verify. The fact is that if Doc James was suddenly to disappear, we might be left in a situation where nobody but the editor adding the content could verify it. I can get pretty much any book or journal article with an interlibrary loan, fairly conveniently. Asking Doc to check these articles is an unreasonable burden on his time. I don't imagine that UpToDate wants its articles sent electronically either. Practical verifiability is a legitimate concern - certainly not absolutely irrelevant, and all else equal, there's no excuse for using a less accessible source over a source which is accessible. Someone who consistently uses inaccessible sources is not following best practices and they should be reminded of that. II | (t - c) 22:48, 4 May 2010 (UTC)
Merge of food allergy and protein allergy
We are discussing the merge of these two pages here: Talk:Protein_allergy#Merge. Comments would be appreciated.Doc James (talk · contribs · email) 18:54, 2 May 2010 (UTC)
- "merged"Doc James (talk · contribs · email) 18:46, 4 May 2010 (UTC)
An editor with a chip on their shoulder (see their possibly forbidden username) has made an edit that has been reverted. That article may need to be gone through to make sure it lives up to our MEDRS guideline. -- Brangifer (talk) 00:04, 3 May 2010 (UTC)
Would someone create a stub on the term rubeosis?? Thanks in advance! ---kilbad (talk) 23:55, 3 May 2010 (UTC)
- Do you mean just reddening of the skin, or are you referring to rubeosis iridis, a specific pathology causing reddening of the iris from neovascularization after surgery or trauma? SBHarris
- The term as used in this list. ---kilbad (talk) 20:45, 5 May 2010 (UTC)
Google editors
I have made a number of suggestion to improving our collaboration with google Wikipedia talk:WikiProject Medicine/Google Project. Comments would be appreciated.Doc James (talk · contribs · email) 06:19, 4 May 2010 (UTC)
- One concern is that a number of google editors are recommending against journals that are not free access. I am not sure how to send a note out to all of them that none free access journals are acceptable.--Doc James (talk · contribs · email) 06:31, 4 May 2010 (UTC)
- Where are these discussions taking place? (Do they need an explanation of the "off-wiki consensus" rule?)
- Fundamentally, I think that we need to use the best available sources, and use paywall issues only to choose between two equally ideal sources. If Google wants a pay-walled paper to be freely available to the world, then that can usually be arranged -- either by Google paying the publisher their open access fee, or by special arrangement with the author (who sometimes hold the copyrights and thus can reproduce the paper on their own websites). WhatamIdoing (talk) 18:08, 4 May 2010 (UTC)
- This is part of the google.org project linked above.Doc James (talk · contribs · email) 18:49, 4 May 2010 (UTC)
- Yes, but how are we communicating with these editors? They're not posting to the Google project page, and they're not posting here. How exactly do you know that they are recommending against paywall journals? Where did they say this? WhatamIdoing (talk) 17:21, 7 May 2010 (UTC)
- This is part of the google.org project linked above.Doc James (talk · contribs · email) 18:49, 4 May 2010 (UTC)
- Here is one comment which says this [8] and it has been stated in one other place. It is unfortunate that these reviews do not seem to be getting involved either here or the google project page.Doc James (talk · contribs · email) 19:05, 7 May 2010 (UTC)
Good point, WAID. I was wondering about where this project is occurring. I keep seeing references to it but no actual messages between WP editors and the Google folks (who, incidentally, mostly (or all?) seem to work for a journal article editing company in North Carolina called American Journal Experts. Isn't this a bit odd?Postpostmod (talk) 00:21, 9 May 2010 (UTC)
- Here is were the discussion is taking place [9] and [10] But some more background on this would be nice. Who are these people who have joined? Are they reimbursed by google? Etc Doc James (talk · contribs · email) 01:51, 10 May 2010 (UTC)
- Well, that's where we're talking... to no one but ourselves, as far as I can tell.
- My guess is that the reviewers (whose efforts I sincerely and deeply appreciate) are only looking at their assigned articles. This means that we're likely to have to explain the same issues to each one, individually, at each and every article, instead of having a centralized communication point for them. In the meantime, I suspect that we need to get a few more people to watchlist some or all of the articles. WhatamIdoing (talk) 03:09, 10 May 2010 (UTC)
- Good idea to get more people to watchlist the articles - but seems like a laborious way to check, for the long haul. Regarding transparency of communication, I posted at the project talk page [11] asking TimV how he's communicating with the editors. I'm not sure if that's the best way to contact him about it, though.Postpostmod (talk) 13:00, 10 May 2010 (UTC)
- Hello everyone, I'm one of those editors, but I am contracted for BioscienceWriters.com (BSW) not AJE. I think those are the only two companies involved right now, but don't quote me on that. BSW just started a trial of 20 articles all from the list on the [12] page. AJE has been reviewing project articles for longer than we have, but that is all I know about their participation. My understanding is that BSW is doing trials edits for about 20 articles and if our reviews are useful to you, there may be a contract for a larger number of articles in the future. The trial review process should take a couple of weeks. We were directed to spend about 2 hours per article, minimize direct edits unless they are simple (like adding citations or citation needed tags) and focus on these areas in order of priority:
- the first priority is to point out inaccuracies
- the second is probably to point out important missing information
- the third is to focus on more complete citations
- But collaborative organization is as follows: a google representative and a [13] representative (TimV) gave us a brief intro via phone conference call, and now all the editors post questions and requests for feedback either to the BSW business manager or directly on the [14] talk page. The BSW manager communicates with the Google and Wiki rep and then gives us feedback. So in essence, we are getting feedback both directly from you via the [15] talk page and indirectly from TimV and a Google representative. I encourage you to communicate your needs and thoughts on the reviews on the [16] talk page and because everyone is reading those. The one discrepancy I've noticed is that talk page participants seem to like more direct edits, while our direction from the project organizers is to minimize those. So I am trying to do a balance between those needs. And yes, Google is footing the cost of the project. Google is also definitely reading that talk page and taking note of your comments there, so make them known! Not sure about this one. Should I cross post this on the project page? BSW-RMH (talk) 15:27, 13 May 2010 (UTC)
- Hello everyone, I'm one of those editors, but I am contracted for BioscienceWriters.com (BSW) not AJE. I think those are the only two companies involved right now, but don't quote me on that. BSW just started a trial of 20 articles all from the list on the [12] page. AJE has been reviewing project articles for longer than we have, but that is all I know about their participation. My understanding is that BSW is doing trials edits for about 20 articles and if our reviews are useful to you, there may be a contract for a larger number of articles in the future. The trial review process should take a couple of weeks. We were directed to spend about 2 hours per article, minimize direct edits unless they are simple (like adding citations or citation needed tags) and focus on these areas in order of priority:
- Good idea to get more people to watchlist the articles - but seems like a laborious way to check, for the long haul. Regarding transparency of communication, I posted at the project talk page [11] asking TimV how he's communicating with the editors. I'm not sure if that's the best way to contact him about it, though.Postpostmod (talk) 13:00, 10 May 2010 (UTC)
- Here is were the discussion is taking place [9] and [10] But some more background on this would be nice. Who are these people who have joined? Are they reimbursed by google? Etc Doc James (talk · contribs · email) 01:51, 10 May 2010 (UTC)
We have a page called Münchausen by Internet which is currently listed as a GA under the WP:MED project. It gets 8 pubmed hits. Wondering if other could take a look? --Doc James (talk · contribs · email) 12:21, 4 May 2010 (UTC)
- Pretending to be someone that you aren't is a social phenomenon, not merely a medical one, so I don't think that PubMed hits is the obvious measure of its notability. WhatamIdoing (talk) 17:35, 4 May 2010 (UTC)
- I think that this is a notible article. I know people who have been victims of what is described in that article and there has been some high profile cases in the media over the years. The sourcing will not be able to reach the standard of well researched disorders such as alziehmers, alcoholism or asthma etc but that is just the name of the game; we do our best using the best available sources on the subject matter, which may be substandard for certain disorders or phenomena.--Literaturegeek | T@1k? 17:35, 7 May 2010 (UTC)
- I am impressed by the quality of the article. It is good enough to make me wonder if it was published elsewhere. alteripse (talk) 22:29, 7 May 2010 (UTC)
- If it was, I can't find any sign of it online. One simple method of looking for plagiarism is to search Google for unusual phrases, such as "development of factitious disorders in online venues" or "monk with end-stage cancer". The only results are obvious mirrors of Wikipedia, such as Nethelper.com. I'd guess that it's simply a well-written article. --RexxS (talk) 01:38, 8 May 2010 (UTC)
Platelet#Activation could be improved/in sync with Coagulation?
Hi all, First off please correct me if it's wrong to ask for improvements in this manner. I'm just looking through the entire platelet activation process in detail and I notice that there seems to be some considerable difference in manner between the coagulation article and the platelet activation subsection. Personally I find the coagulation article much clearer, and in better depth. I'm wondering if maybe the platelet article be brought up to this level, or perhaps a see also marker be placed in the section and a broad overview given instead. At the present time I just found it to be slightly poor compared to the usual standard on these topics. I'm not well enough accustomed to wiki (or endowed with enough knowledge on the topic) to edit it to a suitable standard I feel. Any thoughts? FruitywS (talk) 15:20, 4 May 2010 (UTC)
- Welcome to Wikipedia. Would be happy to help you get access to good journal article and / or textbooks to aid you in improving this article. Google books will often give partial access to recent textbooks well if you find journal you need we here can usually help you get an electronic copy. Doc James (talk · contribs · email) 18:52, 4 May 2010 (UTC)
I've begun an article on Save the Children's State of the World's Mothers report. This year's report seems of particular relevance to upcoming events at the 36th G8 summit. I've just proposed a rather provocative T:DYK hook for it, which unfortunately seems to be true however preposterous it might sound:
- ... that Save the Children's State of the World's Mothers report ranked the U.S. 28th, citing a lifetime risk of maternal death five times greater in the U.S. than in Bosnia and Herzegovina?
I would welcome your insights. Mike Serfas (talk) 02:18, 7 May 2010 (UTC)
- Data would look best turned into the form of maps. There is a guy over at Wikimedia who has help me generate alot of maps who would probably be willing to help. [17] Doc James (talk · contribs · email) 02:30, 7 May 2010 (UTC)
- I thought about making the .svg map for the set of 57 countries with critical shortages of healthcare workers shown in the report. Also, I suppose some of the statistics (child mortality) might be bracketed and colorized. Is that what you mean? (I know how to do this, but thanks) Mike Serfas (talk) 02:49, 7 May 2010 (UTC)
- Here is an example of such a map [18] One could create on for mortality. It would give a quick world wide comparison of rates in different areas of the globe. Africa would of course light up. Doc James (talk · contribs · email) 15:10, 7 May 2010 (UTC)
![[18]](https://commons.wikimedia.org/wiki/File:Unipolar_depressive_disorders_world_map_-_DALY_-_WHO2002.svg){kind=link}
Could someone with experience in the area of anesthetics please have a look at the recent IP edits to isoflurane? They are presumably well-intentioned, but made by a someone whose native language is probably not English. Also, though this is not my area of expertise, I suspect there may be some over-interpretation of the cited references. ChemNerd (talk) 11:43, 7 May 2010 (UTC)
- I have no medical experience of anesthetics, as I am not an MD, but I have when reading through refs when working midazolam to GA status, found several references which discussed the neurotoxicity potential of general anesthetics. However, they were all talking about the neonate (and I think also pregnancy), causing apoptosis at doses equivalent to those used in humans. The FDA is currently investigating these issues. The two worst offenders were isoflurane and ketamine but all GABAergic and NMDA antagonist drugs seem implicated and combining anesthetic agents, eg giving a premed of midazolam or nitrous oxide with for example isoflurane appears to enhance the degree of apoptosis. With regard to the elderly, I did speak to a doctor who said that post-operative cogitive decline is fairly common and can be short-lasting or long-lasting. So it seems the very young and the elderly are more vulnerable to the effects of general anesthetics. I did do some rewriting and deleted and added some text. The sourcing for that section is not the best and if anyone wants to take the time to find recent reviews on post-operative decline it would be of value; I may do so when I get a chance.--Literaturegeek | T@1k? 11:19, 8 May 2010 (UTC)
- Thanks for taking a look and thanks for your improvements to the article. ChemNerd (talk) 14:23, 12 May 2010 (UTC)
Harm reduction
It looks like there's a relatively civil POV battle at Harm reduction, and it might be helpful to have more editors adding their comments. Most of it revolves around the drug policies in Sweden, so if there's anyone who reads Swedish or is familiar with their program, your involvement would be especially helpful.
The dispute largely involves the need to accurately interpreting sources (without going well beyond them), so I suspect that many of our editors could be helpful. WhatamIdoing (talk) 17:30, 7 May 2010 (UTC)
This page redirected to xeroderma pigmentosum, but it's not the same syndrome. I have thought opportune to cancel the redirect... I'm waiting for someone of you who can be engaged to write a more complete voice. --Ceccomaster (talk) 14:16, 8 May 2010 (UTC)
- I made a stub. ---kilbad (talk) 14:33, 8 May 2010 (UTC)
Looking for citations
I see on alexa.com that Wikipedia is ranked at #6. Are there any other references, perhaps from a scientific journal, etc., available that I can site relative rank of Wikipedia among other top websites? I would prefer to cite something other than alexa if possible. ---kilbad (talk) 15:18, 8 May 2010 (UTC)
- I don't think that it is necessary to use a scientific journal as it is not a scientific statement you are trying to make but more just a statistical fact. Any secondary source, perhaps one discussing web trends could be used? If not then Alexa I think would be ok, it is not really controversial what you are wanting to state.--Literaturegeek | T@1k? 15:24, 8 May 2010 (UTC)
- Also, is stats.grok.se the best place to get page view statistics? Is there anywhere I can get some background information on what grok.se is all about? ---kilbad (talk) 16:01, 8 May 2010 (UTC)
- Yea, stats.grok.se tells you basically how many people have viewed an article page per day, week or month. I am not aware off the top of my head of any other tools for generating page view statistics. You can read more about it on their "about" page.--Literaturegeek | T@1k? 17:37, 8 May 2010 (UTC)
- Also, is stats.grok.se the best place to get page view statistics? Is there anywhere I can get some background information on what grok.se is all about? ---kilbad (talk) 16:01, 8 May 2010 (UTC)
Will someone merge histories
Initially, the list of cutaneous condition was found at a different location than it is now. Initially, the list was found at what is now called "cutaneous conditions." However, after various moves and renames, the list if now at "list of cutaneous conditions." However, the history of the list is fractured, and I wanted to know if someone could tidy up the histories somehow? If that is even possible? Basically, I would like to see the history of edits starting from here to here moved over to the beginning of the history of the list of cutaneous conditions. Is that possible? I just want to be able to track the history of the development of the list in one place. ---kilbad (talk) 17:18, 8 May 2010 (UTC)
- I dont this is doable, we tried to do it previously, and admins confirmed that it cannot be done MaenK.A.Talk 16:05, 10 May 2010 (UTC)
Is it possible to find...
Is it possible to find the number of new pages created within a certain time frame which are within the scope of a particular project. Restated, and more specifically, if I wanted to know how many new dermatology-related articles had been created since Nov 08, how could I find that out? Could I use the derm assessment data somehow? ---kilbad (talk) 19:05, 8 May 2010 (UTC)
- You probably need a query using the toolserver. User:Mzmcbride is the first name that springs to mind as someone who could tell you either if it's possible or where is best to request the information. --RexxS (talk) 19:59, 8 May 2010 (UTC)
- You might also look into User:AlexNewArtBot/MedicineSearchResult. It might be the closest thing that we currently have to what you want. WhatamIdoing (talk) 01:16, 9 May 2010 (UTC)
Craniosacral therapy pseudoscience needs fixing
http://en.wikipedia.org/wiki/Craniosacral_therapy#The_primary_respiratory_mechanism
This has been tagged for some time and needs to be brought up to MEDRS standards. -- Brangifer (talk) 23:10, 9 May 2010 (UTC)
Can you help me generate this data?
First, for pages within the scope of the Dermatology task force, I am looking to get a listing of articles that are either good or featured status, and the date at which they were given that status. Second, I am looking for some data stating how many derm-related pages have images, and how many do not. Could someone help me with this? Thanks in advance! ---kilbad (talk) 16:06, 10 May 2010 (UTC)
- There are 10 GA, 1 FA and 1 FL [19] Here is the list of GA [20]. Do not know about images. Doc James (talk · contribs · email) 16:11, 10 May 2010 (UTC)
- If you give me a list of "derm-related pages", I can get the # of pages with images and pull the images for you. MastCell Talk 17:41, 10 May 2010 (UTC)
- All the pages are list within the Category:Dermatology_task_force_articles. Can you use that? ---kilbad (talk) 17:47, 10 May 2010 (UTC)
- Or, here is a listing with 1000 results per page: [21] ---kilbad (talk) 17:51, 10 May 2010 (UTC)
- I can use the category - it should be straightforward to work up a script to pull all of the categorized articles, and then mine them for images. MastCell Talk 17:55, 10 May 2010 (UTC)
- Can we somehow compare the number of photos present now, as compared with October 2008, before the derm taskforce was started? ---kilbad (talk) 17:59, 10 May 2010 (UTC)
- It could be done, but would take a bit more work. Basically, you could use the API to pull the last page revision before October 1, 2008, and compare the number of images to the current page revision. It's a bit iffy since Wikipedia is sort of a moving target, and there are probably a lot of articles that weren't around back in 10/08... but if you're interested, it shouldn't require more than a bit of tinkering. MastCell Talk 23:14, 10 May 2010 (UTC)
- Can we somehow compare the number of photos present now, as compared with October 2008, before the derm taskforce was started? ---kilbad (talk) 17:59, 10 May 2010 (UTC)
- I can use the category - it should be straightforward to work up a script to pull all of the categorized articles, and then mine them for images. MastCell Talk 17:55, 10 May 2010 (UTC)
- Or, here is a listing with 1000 results per page: [21] ---kilbad (talk) 17:51, 10 May 2010 (UTC)
- All the pages are list within the Category:Dermatology_task_force_articles. Can you use that? ---kilbad (talk) 17:47, 10 May 2010 (UTC)
- If you give me a list of "derm-related pages", I can get the # of pages with images and pull the images for you. MastCell Talk 17:41, 10 May 2010 (UTC)
- There are 10 GA, 1 FA and 1 FL [19] Here is the list of GA [20]. Do not know about images. Doc James (talk · contribs · email) 16:11, 10 May 2010 (UTC)
- OK, I've trialed a script to collect the data you're interested in. The results are at User:MastCell/Dermatology Images. (Note that the page is very large, as there are ~2,000 articles tagged, so I don't recommend opening it on a mobile device or over a dialup connection unless you're very patient).
The script I worked up is at User:MastCell/dermimages.py, if anyone cares. The tricky thing is that a lot of pages have non-content images - that is, images from stub templates, maintenance templates, navigation templates, etc. I figure you don't want to count those, so I wrote a set of "excludable" images into the script. The set isn't complete - so I need to go through the output, find the non-content images, and add them by hand to the global exclude list in the script. That will make the count more accurate.
I realized halfway through that you're probably most interested in the raw number of pages without images, which isn't readily available from the output I created. I'll modify the script to total up the # of pages, # with zero images, # with 1 image, # with 2 images, etc... it will be easy, but I'll probably get to it tomorrow. In the meantime, the table of results can be sorted by # of images, but that's probably not a great workaround. MastCell Talk 03:49, 11 May 2010 (UTC)
Someone just created a page for Virginia Livingston, and is using it as a transparent and inappropriate soapbox for her therapies being unjustly maligned, using medically unreliable sources, including extensive use of "personal communication". Any interested editors, I'll be culling and rewriting for a while, but review and input is welcome. WLU (t) (c) Wikipedia's rules:simple/complex 22:03, 11 May 2010 (UTC)
I have done some work on this topic which is now before arbcom. TM makes a number of health claims including improving BP, anxiety, and living forever. A member of Arbcom has concluded that the ongoing debates is "really about conflicting philosophies: on the one hand we have, for want of a better word, mysticism; on the other, rationalism." [22] Wondering if others could comment as this does pertain directly with our topic area. Thanks Doc James (talk · contribs · email) 00:23, 12 May 2010 (UTC)
- It is quite possible that ArbCom does not appreciate the higher standards of sourcing agreed for medical claims in WP:MEDRS. I'm not sure how best to raise the issue with them at this late stage, but I'll think about it and try to formulate another post to the Proposed decision talk page. If any other project members feel strongly about the sourcing issues – and how they may affect us – I'd recommend making your views known there. --RexxS (talk) 02:45, 12 May 2010 (UTC)