An equianalgesic chart is a conversion chart that lists equivalent doses of analgesics (drugs used to relieve pain). Equianalgesic charts are used for calculation of an equivalent dose (a dose which would offer an equal amount of analgesia) between different analgesics.[1] Tables of this general type are also available for NSAIDs, benzodiazepines, depressants, stimulants, anticholinergics and others as well.
Format
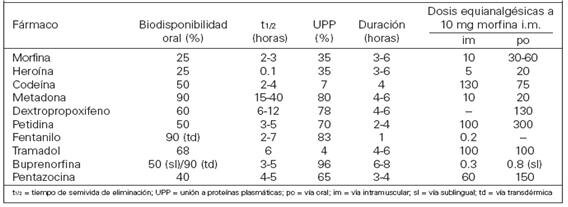
Equianalgesic tables are available in different formats, such as pocket-sized cards for ease of reference.[1] A frequently-seen format has the drug names in the left column, the route of administration in the center columns and any notes in the right column.[2][3]
Purpose
There are several reasons for switching a patient to a different pain medication. These include practical considerations such as lower cost or unavailability of a drug at the patient's preferred pharmacy, or medical reasons such as lack of effectiveness of the current drug or to minimize adverse effects. Some patients request to be switched to a different narcotic due to stigma associated with a particular drug (e.g. a patient refusing methadone due to its association with opioid addiction treatment).[4] Equianalgesic charts are also used when calculating an equivalent dosage of the same drug, but with a different route of administration.
Precautions
An equianalgesic chart can be a useful tool, but the user must take care to correct for all relevant variables such as route of administration, cross tolerance, half-life and the bioavailability of a drug.[5] For example, the narcotic levorphanol is 4–8 times stronger than morphine, but also has a much longer half-life. Simply switching the patient from 40 mg of morphine to 10 mg of levorphanol would be dangerous due to dose accumulation, and hence frequency of administration should also be taken into account.
There are other concerns about equianalgesic charts. Many charts derive their data from studies conducted on opioid-naïve patients. Patients with chronic (rather than acute) pain may respond to analgesia differently. Repeated administration of a medication is also different from single dosing, as many drugs have active metabolites that can build up in the body.[6] Patient variables such as sex, age, and organ function may also influence the effect of the drug on the system. These variables are rarely included in equianalgesic charts.[7][3][8]
Opioid equivalency table
Opioids are a class of compounds that elicit analgesic (pain killing) effects in humans and animals by binding to the µ-opioid receptor within the central nervous system. The following table lists opioid and non-opioid analgesic drugs and their relative potencies. Values for the potencies represent opioids taken orally unless another route of administration is provided. As such, their bioavailabilities differ, and they may be more potent when taken intravenously. Methadone is different from most opioids considering its potency can vary depending on how long it is taken. Acute use, 1–3 days, yields a potency about 1.5× stronger than that of morphine and chronic use (7 days+) yields a potency about 2.5 to 5× that of morphine due to methadone being stored in fat tissue, thus giving higher serum levels with longer use.[citation needed] Similarly, the effect of tramadol increases after consecutive dosing due to the accumulation of its active metabolite and an increase of the oral bioavailability in chronic use; this effect becomes less significant again with even longer use as tolerance develops.[citation needed]
| Opioid Equivalency Table (morphine, oral) [a] | ||||||||
| Analgesic | Strength (relative) |
Equivalent dose (10 mg oral morphine)[b] |
Bioavailability | Half-life of active metabolites (hours) |
Oral-to-parenteral ratio | Speed of onset | Duration | |
|---|---|---|---|---|---|---|---|---|
| Paracetamol (non-opioid) | 1⁄360 | 3600 mg | 63–89% | 1–4 | 37 min (PO); 8 min (IV) | 5 – 6 hours | ||
| Aspirin (NSAID, non-opioid) | 1⁄360 | 3600 mg | 80–100% | 3.1–9 | ||||
| Ibuprofen[10] (NSAID, non-opioid) | 1⁄222 | 2220 mg | 87–100% | 1.3–3 | ||||
| Diflunisal (NSAID, non-opioid) | 1⁄160 | 1600 mg | 80–90% | 8–12 | ||||
| Naproxen[10] (NSAID, non-opioid) | 1⁄138 | 1380 mg | 95% | 12–24 | ||||
| Piroxicam (NSAID non-opioid) | 1⁄120 (est.) | |||||||
| Indomethacin (NSAID non-opioid) | 1⁄64 (est.) | |||||||
| Diclofenac[10][11] (NSAID, non-opioid) | 1⁄14 (est.) | 160 mg (est.) | 50–60% | 1–4 | ||||
| Nefopam (Centrally-acting non-opioid) | 5⁄8 (est.) | |||||||
| Dextropropoxyphene[12] | 1⁄13–1⁄20 | 130–200 mg | ||||||
| Codeine | 1⁄10–3⁄20 | 100–120 mg (PO) | ~90% | 2.5–3 (C6G 1.94;[13] morphine 2–3) | 15–30 min (PO) | 4–6 hours | ||
| Tramadol | 1⁄10 | ~100 mg | 75% (IR), 85–90% (ER) | 6.0–8.8[14] (M1) | ||||
| Opium (oral) | 1⁄10 | ~100 mg | ~25% (morphine) | 2.5–3.0 (morphine, codeine) | ||||
| Tilidine | 1⁄10 | 100 mg | ||||||
| Dihydrocodeine | 1⁄5 | 50 mg | 20% | 4 | ||||
| Anileridine[15] | 1⁄4 | 40 mg | ||||||
| Alphaprodine | 1⁄4–1⁄6 | 40–60 mg | ||||||
| Tapentadol[16] | 3⁄10 | 32 mg | 32% (fasting) | |||||
| Pethidine (meperidine) | 1⁄3 | 30 mg SC/IM/IV, 300 mg (PO) | 50–60% | 3–5 | ||||
| Benzylfentanyl | 1⁄2 | |||||||
| AH-7921 | 4⁄5 | |||||||
| Hydrocodone | 1 | 10 mg | =80% | 3.8–6 | ||||
| Metopon | 1 | 10 mg | ||||||
| Pentazocine lactate (IV)[17] | 1 | 10 mg SC/IV/IM, 150 mg (PO) | ||||||
| Morphine (oral) | 1 | 10 mg | ~25% | 2-4 | 3:1 | 30 min (PO) | 3–5 hours | |
| Oxycodone[18] | 1.5 | 6.67 mg | 60 - 87% | 2 – 3 hours (Instant Release)(PO); 4.5 hours (Controlled Release)(PO) | 10–30 min (Instant Release)(PO); 1 hour (Controlled Release)(PO) | 3 – 6 hours (Instant Release)(PO); 10–12 hours (Controlled Release)(PO)[19] | ||
| Spiradoline | 1.5 | |||||||
| Nicomorphine | 2–3 | 3.33-5 mg | 20% | 4 | ||||
| Morphine (IV/IM) | 3 | 3.33 mg | 100% | 2–3 | 3:1 | 5 min (IV); 15 min (IM) | 3–7 hours | |
| Clonitazene | 3 | 3.33 mg | ||||||
| Methadone (acute)[20][21] | 3–4 | 2.5–3.33 mg | 40–90% | 15–60 | 2:1 | |||
| Methadone (chronic)[21] | 2.5–5 | 3.33 mg | 40–90% | 15–60 | 2:1 | |||
| Phenazocine | 4 | ~2.5 mg | ||||||
| Diamorphine (heroin; IV/IM)[22] | 4–5 | 2–2.5 mg | 100% | <0.6 | Instantaneously (from 5 - 15 sec)(IV); 2 - 5 min (IM) | 4 to 5 hours | ||
| Dezocine | 4–6 | 1.6–2.5 mg | 97% (IM) | 2.2 | ||||
| Hydromorphone[23][24][16] | 10–15 (sc),(iv),(im) 3.75–5 (po) |
0.75 mg (sc,iv,im) 2 mg (po) |
62% | 2–3 | 5:1 | |||
| Oxymorphone[18] | ≤ 3 (PO) *Avoid if possible do to low B.A. same w/ 10% (PO) Buprenorphine 4.5 Sublabial), 4.8 ≈ 5 (Buccal)
5.5 - 6 (Sublingual) 6.3 – (IN) (Intranasal) *13 - 18* (IV, IM ,IO, IT-Spinal, SC , IC & (PCA) [Citation needed] more info coming soon [Under Construction]
|
3.33 mg (PO), 1 mg (IV,IM & Interlaminar
–––––––––– , 0.75 mg IO due to being at the heart & in Intracranial (IC) 0.25 mg - 0.75 mg due to being in the brain *Make sure* ICP Monitor is on W/ avoiding IO & IC if history of Brain Injury or infections, Annuerism Stroke / Hemmorages ,Blood Clots heart Attack , Seizures , M-Dystropy, & Pulmonary /Neurological issues nos use w/ caution ^ ICP w/ms. ||–––Classic opaites. Use with low dose Ketamine to reduce OxyM load for lower complications and better outcomes. |
10%–PO , ≈ 25% Sublabial , ≈ 28% Buccal , (35% - 40%) Sublingual & Intranasal 43% BA. other: rectal Very low ≈ 12.75% New Study & w/ less duration of 3-4 hours. Both PO & Rectal to be avoided do to new studies; and low B.A. More Studies are being conducted do new Fentanyl Drug Bill.
|
7.25–9.43 | 35 min (PO),
–––––––––– 25 min ≈ (Subliabial), 20 Min (Buccal) 15 min or less * Sublingual Side note: for providers [Citation needed] IR Tablets 5mg (Blue / 10 mg Pink) Seems to work best under tongue. (SL|UT): 7.5 - 15 min Buccal: <20 min. (SL|ULL) 13 - 23 min & slower AB. w/ longest Duration of 7-9 hrs. Instantaneously (from 5 - 15 sec)(IV), IM 12.5 - 15 min , IO 2.5 ~ 3 min, IT 3 - 5 min, IN 7 - 11 min IC 1 ~ 2 min Other: Rectal (Try to avoid, unless only option newer methods now used.)
|
5–7 hours
PO / NGT&SGTS –––––––––– (6–8 hours), Transmuccal *Subliabial, (under lip - lower gums) *Buccal *Sublingual –––––––––4-6 Hours:(IV, IM ,IO, IT-Spinal, SC & (PCA) [Citation needed, under construction. | ||
| U-47700 | 7.5 | 1.5 mg | 1.5-3 | |||||
| Levorphanol[25] | 8 | 1.25 mg | 70% | 11–16 | 1:1 | |||
| Desomorphine (Krokodil) | 8–10 | 1–1.25 mg | ~100% (IV) | 2–3 | Instantaneously (from 5 - 15 sec)(IV); 2 - 5 min (IM) | 3 – 4 hours | ||
| N-Phenethylnormorphine | 8–14 | |||||||
| Alfentanyl | 10–25 | 1.5 (90–111 minutes) | Instantaneously (from 5 - 15 sec); 4x more rapid than fentanyl | 0.25 hr (15 min); up to 54 minutes until offset of effects | ||||
| Trefentanil | (10–25)+ | |||||||
| Brifentanil | (10–25)+ | |||||||
| Acetylfentanyl | 15 | |||||||
| 7-Hydroxymitragynine | 17 | ~0.6 mg | ||||||
| Furanylfentanyl | 20 | |||||||
| Butyrfentanyl | 25 | |||||||
| Enadoline | 25 | |||||||
| Buprenorphine (SL)[12] | 40 | 0.25 mg | 30%(SL)[26]; ~100% (TD); 65% (buccal)[27][28]; 48% (INS)[29] | 20–70, mean 37 | 3:1 | 45 min | 12-24 hours | |
| N-Phenethyl-14-ethoxymetopon | 60 | |||||||
| Etonitazene | 60 | 160 µg | ||||||
| Phenomorphan | 60–80 | 0.13–0.16 mg | ||||||
| N-Phenethylnordesomorphine | 85 | |||||||
| Phenaridine | (50–100)− | |||||||
| Fentanyl | 50–100 | 0.1 mg (100 µg) IM/IV | 33% (SL); 92% (TD); 89% (INS); 50% (buc) | 0.04 (IV); 7 (TD) | 5 min (TD/IV) | 30–60 minutes (IV) | ||
| Acrylfentanyl | (50–100+) | |||||||
| Buprenorphine (Transdermal)[30][31] | 100-115 | 0.1mg (100µg) | 30%(SL)[26]; ~100% (TD); 65% (buccal)[27][28]; 48% (INS)[29] | 3:1 | 45-60 minutes | 12-24 hours | ||
| 14-Cinnamoyloxycodeinone | 177 | |||||||
| Remifentanil | 100–200 | 50–100 µg | 0.02 (1-20 minutes) | Instantaneously (from 5 - 15 sec) | 15 minutes; rapid offset of effects necessitates continuous infusion for maintenance of anaesthesia | |||
| Ocfentanil | 125–250 | 40–80 µg | ||||||
| Ro4-1539 | 240–480 | |||||||
| Sufentanil | 500–1,000 | 10–20 µg | 4.4 | |||||
| BDPC | 504 | ~20 µg | ||||||
| C-8813 | 591 | |||||||
| 4-Phenylfentanyl | 800 | |||||||
| 3-Methylfentanyl | 1000–1500 | |||||||
| Etorphine | 1,000–3,000 | 3.3–10 µg | ||||||
| Ohmefentanyl | 6300 | |||||||
| Acetorphine | 8700 | |||||||
| Dihydroetorphine[32] | 1,000–12,000 | 0.83–10 µg (20–40 µg SL) | ||||||
| 2-Fluorohmefentanil | 18,000 | |||||||
| 4-Carboethoxyohmefentanil | 30,000 | |||||||
| R-30490 | (10,000–100,000)− | |||||||
| Carfentanil[33] | 10,000 | 1.0 µg | 7.7 | |||||
| Lofentanil | (10,000–100,000)+ | |||||||
| PO: oral • IV: intravenous injection • IM: intramuscular injection • SC: subcutaneous injection • SL: sublingual • TD: transdermal "Strength" is defined as analgesic potency relative to oral morphine. Tolerance, sensitization, cross-tolerance, metabolism, and hyperalgesia may be complex factors in some individuals. Interactions with other drugs, food and drink, and other factors may increase or decrease the effect of certain analgesics and alter their half-life. Because some listed analgesics are prodrugs or have active metabolites, individual variation in liver enzymes (e.g., CYP2D6 enzyme) may result in significantly altered effects. | ||||||||
Notes
- ^ Approximate. There is a wide range of values in controlled trials[9]
- ^ 10 mg oral morphine is equivalent to n mg analgesic drug x, e.g. 10 mg morphine is equivalent to 3600 mg paracetamol or 1.5 mg hydromorphone
See also
- Oripavine – for more on the comparative strength of oripavine derivatives
References
- ^ a b Joishy 1999.
- ^ McPherson 2009, p. 5.
- ^ a b Natusch 2012.
- ^ McPherson 2009, p. 3.
- ^ McPherson 2009, p. 4.
- ^ McPherson 2009, p. 8.
- ^ McPherson 2009, p. 9.
- ^ Anderson et al 2001.
- ^ Pereira et al 2001.
- ^ a b c "Dosing Guidelines for Acetaminophen and Selected NSAIDs" (PDF). www3.us.elsevierhealth.com.
- ^ http://www.emedexpert.com/compare-meds/diclofenac-vs-naproxen.shtml
- ^ a b "Ch. 4 Narcotics: Synthetic Narcotics: Dextropropoxyphene". Drugs of Abuse. Drug Enforcement Administration, U.S. Department of Justice. 2005. Archived from the original on 2006-11-02.
{{cite book}}: External link in|chapterurl=|chapterurl=ignored (|chapter-url=suggested) (help)CS1 maint: bot: original URL status unknown (link) - ^ KuKanich B (February 2010). "Pharmacokinetics of acetaminophen, codeine, and the codeine metabolites morphine and codeine-6-glucuronide in healthy Greyhound dogs". J. Vet. Pharmacol. Ther. 33 (1): 15–21. doi:10.1111/j.1365-2885.2009.01098.x. PMC 2867071. PMID 20444020.
- ^ "ULTRAM® (tramadol hydrochloride) Tablets Full Prescribing Information" (PDF). US Food and Drug Administration. Ortho-McNeil Pharmaceutical, Inc. March 2008. p. 4. Retrieved December 28, 2016.
The mean terminal plasma elimination half-lives of racemic tramadol and racemic M1 are 6.3 ± 1.4 and 7.4 ± 1.4 hours, respectively. The plasma elimination half-life of racemic tramadol increased from approximately six hours to seven hours upon multiple dosing.
- ^ "Anileridine". DrugBank Version: 3.0. DrugBank.
- ^ a b Cupp 2012.
- ^ "TALWIN (pentazocine lactate) injection, solution". DailyMed. National Institute of Health. Retrieved 2011-12-10.
- ^ a b "Equianalgesic Conversion". GlobalRPH.
- ^ Sunshine, A; Olson, N; Colon, A; Rivera, J; Kaiko, R.F.; Fitzmartin, R.D.; Reder, R.F.; Goldenheim, P.D. (July 1996). "Analgesic Efficacy of Controlled‐Release Oxycodone in Postoperative Pain". Journal of Clinical Pharmacology. 36 (7): 595–603. doi:10.1002/j.1552-4604.1996.tb04223.x. PMID 8844441.
- ^ Tabla de equivalencia opiáceos
- ^ a b Manfredonia JF (March 2005). "Prescribing methadone for pain management in end-of-life care". J Am Osteopath Assoc. 105 (3 Suppl 1): S18–21. PMID 18154194. Table 2: Conversion Ratio of Oral Morphine to Methadone[permanent dead link].
- ^ Reichle CW, Smith GM, Gravenstein JS, Macris SG, Beecher HK (April 1962). "Comparative analgesic potency of heroin and morphine in postoperative patients". J. Pharmacol. Exp. Ther. 136 (1): 43–6. PMID 14491157.
- ^ Toronto Surgery 2014.
- ^ Walker 2001.
- ^ "Levorphanol". DrugBank Version: 3.0. DrugBank.
- ^ a b Mendelson J, Upton RA, Everhart ET, Jacob P 3rd, Jones RT (1997). "Bioavailability of sublingual buprenorphine". Journal of Clinical Pharmacology. 37 (1): 31–7. doi:10.1177/009127009703700106. PMID 9048270
- ^ a b "Buprenorphine / Naloxone Buccal Film (BUNAVAIL) C-III" (PDF). Pharmacy Benefits Management (PBM) Services. September 2014.
{{cite web}}: CS1 maint: url-status (link) - ^ a b BUNAVAIL (buprenorphine and naloxone) buccal film, CIII [prescribing information online]. BioDelivery BioDelivery Sciences International, Inc. (BDSI), Raleigh, NC. Jun 2014.
- ^ a b Eriksen J, Jensen NH, Kamp-Jensen M, Bjarnø H, Friis P, Brewster D (1989). "The systemic availability of buprenorphine administered by nasal spray". J. Pharm. Pharmacol. 41 (11): 803–5. doi:10.1111/j.2042-7158.1989.tb06374.x
- ^ Khanna, IK; Pillarisetti, S (2015). "Buprenorphine - an attractive opioid with underutilized potential in treatment of chronic pain". Journal of pain research. 8: 859–70. doi:10.2147/JPR.S85951. PMID 26672499
- ^ Cote, J; Montgomery, L (July 2014). "Sublingual buprenorphine as an analgesic in chronic pain: a systematic review". Pain medicine (Malden, Mass.). 15 (7): 1171–8. doi:10.1111/pme.12386. PMID 24995716
- ^ Ohmori, Satoshi; Morimoto, Yasunori (2002). "Dihydroetorphine: a potent analgesic: pharmacology, toxicology, pharmacokinetics, and clinical effects". CNS Drug Reviews. 8 (4): 391–404. doi:10.1111/j.1527-3458.2002.tb00236.x. ISSN 1080-563X. PMC 6741694. PMID 12481194.
Dihydroetorphine (DHE) is one of the strongest analgesic opioid alkaloids known; it is 1000 to 12,000 times more potent than morphine. ...
MOR is the most commonly used opioid analgesic for pain relief, and its oral daily dose (20 to 1000 mg) is relatively high (44). On the other hand, DHE produces rapid analgesic effects at an extremely low dose, 20 ìg sublingually in humans (60, 78). ... - ^ "Carfentanil". DrugBank Version: 3.0. DrugBank.
{kind=link}
Bibliography
- Books
- Cupp, Melanie (August 2012). "Equianalgesic Dosing of Opioids for Pain Management. PL Detail-Document #280801" (PDF). Pharmacist's Letter.
{{cite journal}}: Invalid|ref=harv(help) - Joishy, S. K. (1999). Palliative medicine secrets. Philadelphia PA: Hanley & Belfus. p. 97. ISBN 978-1-56053-304-7.
{{cite book}}: Invalid|ref=harv(help) - McCaffery, Margo; Pasero, Chris (1999). Pain: Clinical Manual (2nd ed.). Mosby. ISBN 978-0-8151-5609-3.
{{cite book}}: Invalid|ref=harv(help), Extra information, including printable charts - McPherson, Mary Lynn M. (2009). Demystifying Opioid Conversion Calculations: A Guide for Effective Dosing. Bethesda MD: American Society of Health-System Pharmacists. p. 5. ISBN 978-1-58528-297-5.
{{cite book}}: Invalid|ref=harv(help)
- Articles
- Anderson, Robert; Saiers, Joseph H; Abram, Stephen; Schlicht, Christian (May 2001). "Accuracy in Equianalgesic Dosing". Journal of Pain and Symptom Management. 21 (5): 397–406. doi:10.1016/S0885-3924(01)00271-8. PMID 11369161.
- Natusch, Douglas (February 2012). "Equianalgesic doses of opioids – their use in clinical practice". British Journal of Pain. 6 (1): 43–46. doi:10.1177/2049463712437628. PMC 4590088. PMID 26516465.
{{cite journal}}: Invalid|ref=harv(help) - Pereira, Jose; Lawlor, Peter; Vigano, Antonio; Dorgan, Marlene; Bruera, Eduardo (August 2001). "Equianalgesic Dose Ratios for Opioids". Journal of Pain and Symptom Management. 22 (2): 672–687. doi:10.1016/s0885-3924(01)00294-9. PMID 11495714.
- Websites
- "Opioid Equianalgesic Table". Lecture Notes. Department of Surgery, University of Toronto. November 2014. Retrieved 26 February 2020.
- Walker, Paul (2001). "Issue 17. Morphine vs Hydromorphone vs Oxycodone vs The Patch". Palliative Care Tips: Info for Health Professionals. Palliative & End of Life Care (PEOLC), Alberta Health Services. Archived from the original on December 24, 2001.
{{cite web}}: Invalid|ref=harv(help) - "Management of Opioid Therapy (OT) for Chronic Pain (2017)" (PDF). VA/DoD Clinical Practice Guidelines. Department of Veterans Affairs. p. 99. Retrieved 26 February 2020.
- Online opioid equianalgesia calculator Electronic calculator that includes logic for bidirectional and dose-dependent conversions
- Opioid equianalgesic tables: are they all equally dangerous?